Robert E. Marx - Oral Pathology in Clinical Dental Practice
Здесь есть возможность читать онлайн «Robert E. Marx - Oral Pathology in Clinical Dental Practice» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Oral Pathology in Clinical Dental Practice
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Oral Pathology in Clinical Dental Practice: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Oral Pathology in Clinical Dental Practice»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Oral Pathology in Clinical Dental Practice — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Oral Pathology in Clinical Dental Practice», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Radiographic presentation
None.
Differential diagnosis
The acute phase may be identical to a drug-induced mucositis from chemotherapy, which may have been used concomitant with the radiotherapy. Otherwise, consider secondary mucositis from HIV, leukemia, or multiple myeloma. The chronic phase will resemble a chemical burn such as lye ingestion or progressive systemic sclerosis (scleroderma).
Microscopic features
The acute phase will show hyperemia and sludging in most vessels as well as interstitial edema and acute inflammatory cells. The chronic phase will be poorly vascular and poorly cellular with collagen replacing most cellular elements as seen in a scar.
Suggested course of action
During the acute phase, advise the patient to avoid alcohol or acid-containing medicaments and foods. Prescribe “magic mouthwash”—ie, Kaopectate (Chattem) 5 mL, Benadryl (McNeil) 12.5 mg, and dexamethasone 12 mg swish and spit—and/or 2% lidocaine gel to be applied topically before meals and as needed. If secondary infection is suspected (eg, tender lymphadenopathy, significant mucosal pain), also treat with antibiotics: amoxicillin 500 mg three times daily or doxycycline 100 mg daily.
Treatment
No specific curative treatment is known. However, the palliative care discussed above is useful.
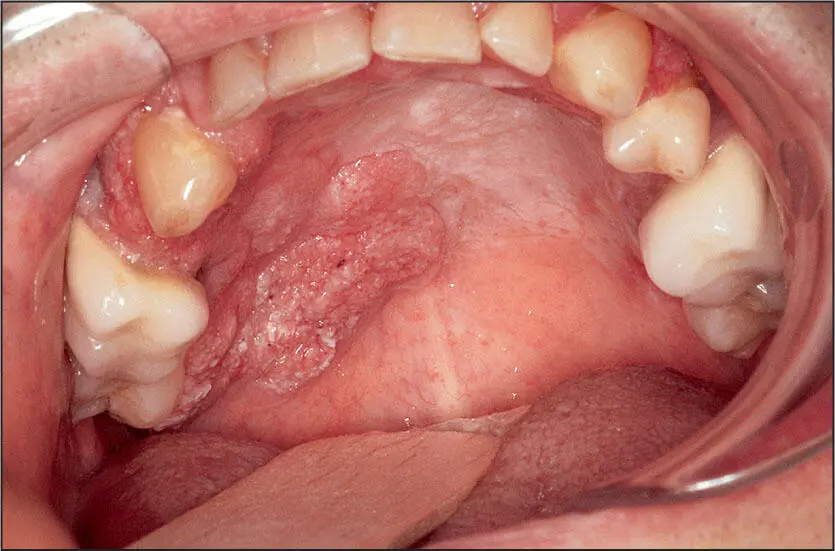
 Widespread surface involvement of dysplasia/carcinoma in situ and invasive carcinoma.
Widespread surface involvement of dysplasia/carcinoma in situ and invasive carcinoma.
Field Cancerization
Nature of disease
Although smoking and certain human papillomaviruses (HPV) have been linked to oral squamous cell carcinoma, a significant number occur without any apparent carcinogen exposure. One of these is the field cancerization phenomenon in which the normal oral mucosa transforms into squamous cell carcinoma over a wide area and with new lesions developing over time.
Predilections
Adults over 30 years of age, with a slight female predilection. No racial predilection is known.
Clinical features
Pebble-like leukoplakia or erythroplakia over a wide surface area, mostly seen on the gingiva, at the lateral border of the tongue, and on the buccal mucosa. This condition is often painful and does not develop ulcerations or regional lymph node spread until it has been present for some time.
Radiographic presentation
Radiographs are usually normal until late in its course, when bony invasion results in osteolysis.
Differential diagnosis
Proliferative verrucous leukoplakia bears a very close resemblance to field cancerization and is actually another form of it, but one that goes through a verrucous phase (while field cancerization does not). Additionally, lichen planus, candidiasis, and a large isolated T3 squamous cell carcinoma may be considered.
Microscopic features
Field cancerization histopathology is no different than that of isolated dysplasia, carcinoma in situ, and invasive squamous cell carcinoma that represent focal disease, in which atypical epithelial cells with pleomorphic nuclei and mitotic figures occur above an intact basement membrane and then invade through the basement membrane to the subjacent connective tissue, sometimes forming keratin pearls and other times more anaplastic features.
Suggested course of action
Suspicious cases should be photographed for documentation and biopsied. If this cannot be accomplished by the initial examining practitioner, the patient should be referred to an oral and maxillofacial surgeon or a regional cancer center.
Treatment
The lesions present at the time are excised with 1.5-cm margins with frozen section control, and the defect is skin grafted or reconstructed with a tissue flap. A prophylactic neck lymphadenectomy is also usually accomplished. If lymphadenopathy is present, a treatment neck dissection is performed. Close follow-up is observed every 2 to 3 months, with retreatment of new lesions as they arise.
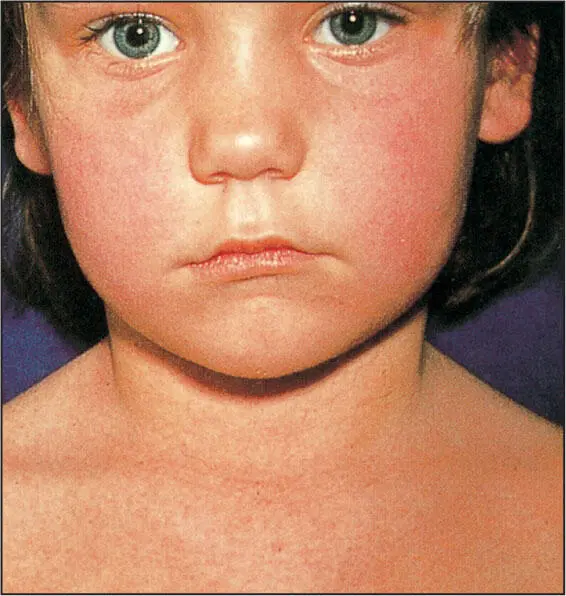
Red macular skin rash seen in scarlet fever.
Scarlet Fever
Nature of disease
Today, a rare bacterial infection caused by group A beta-hemolytic streptococci ( Streptococcus scarlatina or Streptococcus pyogenes ) that produces a unique red macular skin rash and a red swollen tongue by virtue of its erythrotoxin elaboration.
Predilections
Mostly children and young adults. No sex or racial predilection is known.
Clinical features
The child or young adult will present with fever, a sore throat, and headache. The red macular skin rash may appear on the face but will be more prominent in the axillary and groin areas. The tongue will be swollen with reddened fungiform papillae standing out against a white coat on the tongue. This is referred to as “raspberry tongue.”
Radiographic presentation
None.
Differential diagnosis
Other infections such as nonspecific streptococcal pharyngitis, infectious mononucleosis, and pseudomembranous pharyngitis should be considered.
Microscopic features
Tissue specimens are rarely taken as they show a nonspecific inflammatory cell infiltrate with prominent endothelial lysis, dilation of small blood vessels, and hyperemia.
Suggested course of action
Throat cultures of suspicious cases should be taken and a referral made to an infectious disease specialist.
Treatment
Penicillin is the drug of choice: either phenoxymethylpenicillin 500 mg orally four times daily for 10 days or one intramuscular dose of benzathine penicillin 1.2 million units. For penicillin-allergic patients, oral erythromycin 500 mg four times daily or 40 mg/kg per day for 10 days for children is prescribed.
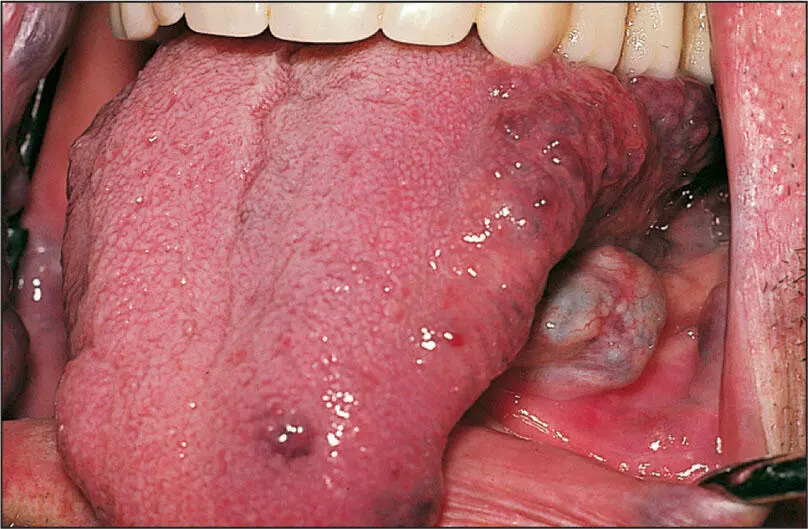
Classic Kaposi sarcoma.

AIDS-related Kaposi sarcoma.
Kaposi Sarcoma
Nature of disease
A low-grade multifocal vascular malignancy due to a viral infection in an individual with a genetic HLA-DR5 antigen predisposition.
Predilections
There are four types of Kaposi sarcoma:
1. Classic Kaposi sarcoma: This type affects mostly men over 60 years of age and has a strong predilection for those of Greek, Italian, or Jewish ethnicity.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Oral Pathology in Clinical Dental Practice»
Представляем Вашему вниманию похожие книги на «Oral Pathology in Clinical Dental Practice» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Oral Pathology in Clinical Dental Practice» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.