Robert E. Marx - Oral Pathology in Clinical Dental Practice
Здесь есть возможность читать онлайн «Robert E. Marx - Oral Pathology in Clinical Dental Practice» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Oral Pathology in Clinical Dental Practice
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Oral Pathology in Clinical Dental Practice: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Oral Pathology in Clinical Dental Practice»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Oral Pathology in Clinical Dental Practice — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Oral Pathology in Clinical Dental Practice», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The white oral and skin lesions may resemble an early case of keratosis follicularis or pachyonychia congenita. Systemic candidiasis or lichen planus with oral and skin lesions may also be considered.
Microscopic features
White patches will show acanthosis and hyperkeratosis. Discolored lesions will show melanin pigment within macrophages and free melanin in the dermis, hence the name incontinentia pigmenti .
Suggested course of action
Suspected cases should be referred to a dermatologist and/or a geneticist.
Treatment
No treatment is required.

 Early PVL of tongue: Field development of lesion.
Early PVL of tongue: Field development of lesion.

Later stage of PVL with widespread involvement of invasive squamous cell carcinoma.
Proliferative Verrucous Leukoplakia (PVL)
Nature of disease
A relentless progression from benign-appearing leukoplakia of only hyperkeratosis through to verrucous hyperplasia, verrucous carcinoma, invasive squamous cell carcinoma, and a final stage of an extremely aggressive and treatment-resistant squamous cell carcinoma.
Predilections
Adults over 50 years. Affects women more than men. Unrelated to tobacco products and high-risk human papillomaviruses. No racial predilection is known.
Clinical features
Depending on the stage and advancement of this disease, it may appear as a large surface area of leukoplakia or multiple exophytic verrucous lesions or a large tumor mass. As many as 90% of patients will have a skin and/or nail fungal condition as well as oral candidiasis.
Radiographic presentation
None until its later stages, when it invades bone to produce an irregular osteolysis.
Differential diagnosis
In its early and intermediate stages, PVL will appear similar to candidiasis and lichen planus. As it progresses, verrucous carcinoma unrelated to PVL and hypertrophic candidiasis may be considered. In its aggressive late stage, invasive squamous cell carcinoma unrelated to PVL and high-grade mucoepidermoid carcinoma and other high-grade cancers are considerations.
Microscopic features
Early stages will show a range from normal-appearing epithelium to varying degrees of dysplasia. A peculiar bulbous endophytic protrusion of epithelium with an intact basement membrane is often seen. In intermediate stages, a verrucous proliferation is noted. In later stages, an invasive squamous cell carcinoma with abundant mitotic figures is seen.
Suggested course of action
Suspicious cases should undergo an incisional biopsy and/or referral to an oral and maxillofacial surgeon.
Treatment
Initially, areas of clinical involvement are excised and skin grafted. Follow-up chemoprevention is not curative but slows down the progression of the disease. Oral nystatin swish and spit, oral-systemic griseofulvin 250 mg twice daily, and tocopherol 100 mcg daily are often used as chemoprevention. Advanced cases are treated with resection and sometimes chemotherapy or radiotherapy, although their value is uncertain.
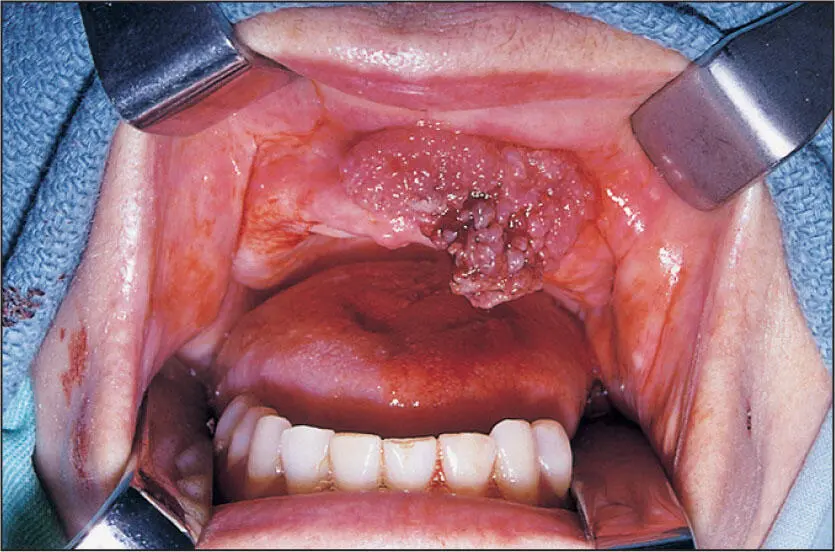
Exophytic verrucous carcinoma of the anterior maxilla in a patient who smoked one pack of cigarettes per day and did not use smokeless tobacco.
Verrucous Carcinoma
Nature of disease
A noninvasive and nonmetastasizing exophytic proliferation of malignant epithelial cells. Note: Although often attributed to smokeless tobacco use, there is no clear evidence that smokeless tobacco other than betel nut/slaked lime causes verrucous carcinoma.
Predilections
Mostly adults over 50 years of age. Slightly more common in males than in females and mostly occurs on the buccal mucosa or gingiva. No racial predilection is known.
Clinical features
Lesions will appear as red-white velvet-textured exophytic masses arising from a broad surface area. Satellite lesions are common. Lesions are asymptomatic without induration or suspicious lymphadenopathy.
Radiographic presentation
None.
Differential diagnosis
Benign hyperkeratosis, squamous papillomas, and invasive squamous cell carcinoma should be considered. Hypertrophic candidiasis and lichen planus may also be considered.
Microscopic features
Bulbous endophytic and exophytic epithelial proliferations are seen together with an intact basement membrane and subjacent inflammation in the mucosa beneath the basement membrane. There are usually clefts with a hyperparakeratinization between the broad exophytic proliferations.
Suggested course of action
Incisional biopsy to include at least one margin and a depth into bleeding submucosa and/or referral to an oral and maxillofacial surgeon.
Treatment
Wide local excision into the submucosa while observing a 1.0- to 1.5-cm margin controlled by frozen sections.

Reddened oral mucosa and gingiva from the yellow dye (tartrazine) in some Synthroid tablets (AbbVie).
Hypersensitivity Mucositis
Nature of disease
An immune-based inflammatory response to topical or systemic agents.
Predilections
Can occur at any age but is mostly seen in adults taking systemic medications. May also be attributed to some ingredients in dental preparations or to food spices. Systemic medications most well known to cause oral hypersensitivity lesions are thyroid-replacement and anti-hypertension drugs. Topical agents more commonly associated with mucosal reactions are common flavoring and nickel-containing materials. No sex or racial predilection is known.
Clinical features
Lesions will be flat, erythematous patches with mild to moderate pain. Certain acidic juices and spices may incite a higher level of pain.
Radiographic presentation
None.
Differential diagnosis
Painful, red oral mucosal lesions suggest pemphigus, erosive lichen planus, and pemphigoid as the most serious considerations. However, a premalignant field dysplasia or field cancer should also be considered.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Oral Pathology in Clinical Dental Practice»
Представляем Вашему вниманию похожие книги на «Oral Pathology in Clinical Dental Practice» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Oral Pathology in Clinical Dental Practice» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.