David Linden - Touch
Здесь есть возможность читать онлайн «David Linden - Touch» весь текст электронной книги совершенно бесплатно (целиком полную версию без сокращений). В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Год выпуска: 2014, ISBN: 2014, Издательство: Penguin Books Ltd, Жанр: Психология, Биология, sci_popular, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Touch
- Автор:
- Издательство:Penguin Books Ltd
- Жанр:
- Год:2014
- ISBN:9780241184059
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Touch: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Touch»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Dual-function receptors in our skin make mint feel cool and chili peppers hot. Without the brain’s dedicated centers for emotional touch, an orgasm would feel more like a sneeze—convulsive, but not especially nice. From skin to nerves to brain, the organization of our body’s touch circuits is a complex and often counterintuitive system that affects everything from our social interactions to our general health and development.
In Touch, neuroscientist and bestselling author David J. Linden explores this critical interface between our bodies and the outside world, between ourselves and others. Along the way, he answers such questions as: Why do women have more refined detection with their fingertips than men? Is there a biological basis for the use of acupuncture to relieve pain? How do drugs like Ecstasy heighten and motivate sensual touch? Why can’t we tickle ourselves? Linking biology and behavioral science, Touch offers an entertaining and enlightening answer to how we feel in every sense of the word.
Touch — читать онлайн бесплатно полную книгу (весь текст) целиком
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Touch», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
I love boozy, geeky conversations in which people drop their inhibitions and consider subjects that might seem silly but actually raise substantive points. Years ago I was talking with my nonscientist friend Q. about tactile sense, and she asked the following wonderful question: If you’re a blind Braille reader and you’ve lost your fingers, could you read with other sensitive skin areas, like the genitals? After all, she said, they do produce a strong sensation in response to light touch. The answer I gave her is that the genitals (both the glabrous and the hairy parts, both male and female) are sensitive , in that they can detect tiny skin indentations. However, they are not finely discriminative , meaning that they do not allow for determination of the precise location, texture, or form of objects pressed against the skin. These regions fail at fine discriminative touch because they are poorly endowed with the shallow touch sensors, most notably the Merkel disks.
Q. was skeptical of my explanation, and so, after quizzing me on experimental design, she decided to perform her own investigation. She gathered a compass with blunted points, a blindfold, and a willing accomplice (her husband). His job was to repeatedly press the compass points gently into her labia minora, varying the gap from 1 to 20 millimeters, and recording whether she perceived the stimulus as a single point or two separate points. This is a standard technique for mapping the skin and is called a two-point discrimination threshold test. Then the tables were turned, and she did the same on her husband’s penis. 32The kinky results: The two-point discrimination threshold on her labia minora was approximately 7 millimeters. On his penis, it was 5 millimeters on the glabrous skin of the glans and 12 millimeters on the hairy skin of the shaft. This compares to a typical value of 1 millimeter on the fingertip and establishes that crotch-based Braille reading will fail. However, not all erogenous zones have poor discrimination of spatial detail. The lips and tongue, by virtue of having a high density of Merkel endings, have superb spatial resolution and hence can be used to read Braille. 33
The typical neuron has a cell body, which contains the DNA-packed nucleus and other organelles, and two different types of projecting fiber, dendrites and axons. The dendrite, a branched signal-receiving structure, passively conducts electrical signals through the cell body to the axon, the information-sending part of the neuron. There is a specialized zone at the start of the axon that can trigger all-or-none signals, the spikes. These spikes can be propagated in a regenerative fashion (like a flame moving down a fuse, igniting the next segment of fuse continually) over long distances. When the spike reaches the terminal end of the axon, it triggers, through a series of rapid biochemical steps, the release of a chemical neurotransmitter that diffuses across a tiny fluid-filled gap to activate specialized neurotransmitter receptors in the dendrite of the next neuron. This connection between neurons is called the synapse. The process by which electrical signals are converted into chemical signals and then back again into electrical signals in the receiving neuron is called synaptic transmission.
The neurons that convey tactile information from the skin to the spinal cord and brain do not have this typical dendrite–cell body–axon shape. Instead, they have a single long axon running from the spot in the skin they sense to the spinal cord. The cell body is attached to the axon by a little stub, tucked off to the side. The cell bodies of many sensory neurons are clumped together in a structure called the dorsal root ganglion, which lies just outside the spinal cord (figure 2.6). There are many pairs of dorsal root ganglia (one on each side of the body), each pair associated with one of the stacked spinal bones called vertebrae. 34
When we think of electrical signaling, we imagine impulses in our laptop computers or iPods, which move at a speed slightly slower than the speed of light, about 669 million miles per hour. Transmission of electrical spikes in the nervous system is a much, much slower process. The axons that carry information from your skin mechanoreceptors can convey spikes at about 150 miles per hour (70 meters per second). These are some of the faster axons in the nervous system, yet they are still more than four-million-fold slower than signals in electronic devices. Or, in other words, imagine if a giant were lying with her head in Baltimore and her foot dangling in the waters off Cape Town, South Africa. If she were brushed on her big toe by a frond of seaweed on Monday at noon, activating her skin mechanoreceptors, she wouldn’t feel it until Wednesday in the midafternoon, when the signal would reach the neocortex of her brain, and she wouldn’t be able to twitch her foot in response until early Saturday. 35Leaving giants aside for a moment, the key point is that it takes time for electrical signals that begin in the skin to propagate to the brain, where they are perceived, and it takes longer for these signals to travel from distant parts of the body, like the toes, than from closer locations, like the face.
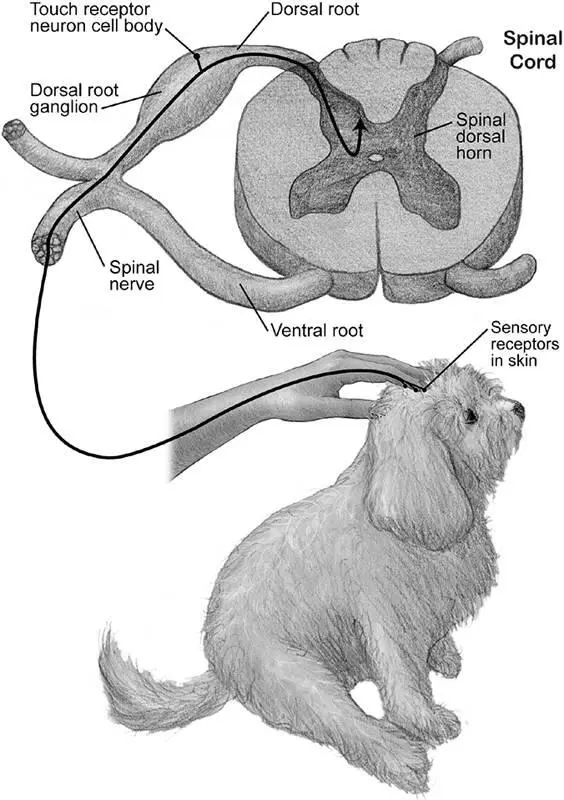
Figure 2.6Electrical signals from sensors in the skin are conveyed to the spinal cord and from there to the brain (upward arrowhead) along the axons of neurons whose cell bodies reside in the dorsal root ganglia. © 2013 Joan M. K. Tycko

At the turn of the twentieth century, some Europeans and Americans, mostly women, would go to the doctor reporting that they had lost touch sensation in a particular region of the body—only a weird, vague tingling remained. Is there a neurological explanation for these symptoms? We know that nerves to the spinal cord and brain convey tactile signals. So might the problem have been that something was interfering with the functioning of a particular sensory nerve—pinching or an infection, perhaps—and it was this disruption that gave rise to a localized numbness? Figure 2.7 shows an image of the human body drawn so that the skin territory innervated by each pair of dorsal root ganglia (one on the left and one on the right) is mapped upon it. For example, you can see that the fourth thoracic dorsal root ganglia carry sensations from a horizontal band of skin that wraps around the torso at the level of the nipples, while the first sacral ganglia, lower down in the spinal column, innervate vertical stripes running down the outside of the calf, ankle, and foot. Each of these skin regions innervated by a pair of dorsal root ganglia is called a dermatome.
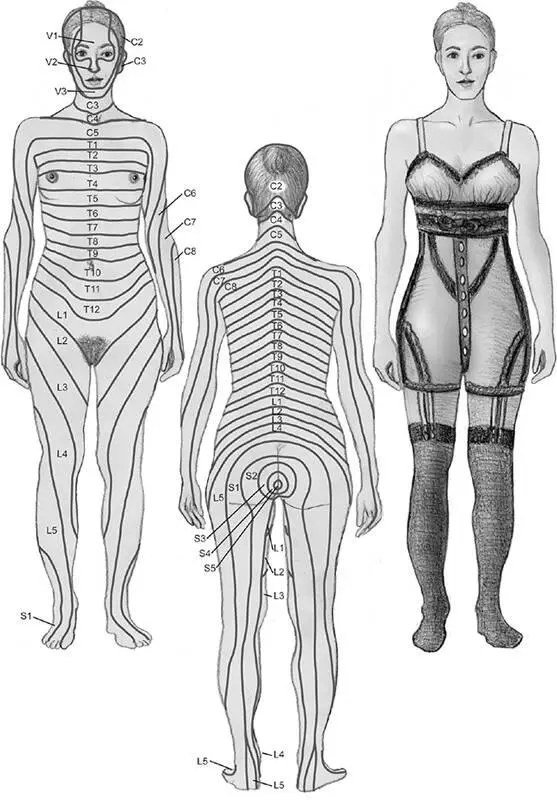
Figure 2.7A map of skin regions innervated by fibers from various spinal nerves and the trigeminal nerve serving parts of the face. This map (left and center) shows that these dermatomes do not correspond to the underwear-shaped regions of numbness (right) widely reported by female patients at the turn of the twentieth century. The letters S, L, T, and C correspond to groups of vertebrae, ranging from the bottom to the top of the spinal cord: sacral, lumbar, thoracic, and cervical. The letter V denotes the trigeminal nerve, which originates from the brain stem. It is the fifth cranial nerve, hence it is designated by the Roman V. © 2013 Joan M. K. Tycko
If trauma to a sensory nerve or a dorsal root ganglion were the cause of these tingly symptoms, one would imagine that the reported area of numbness would have the shape of a dermatome (or maybe two adjacent dermatomes). However, when the doctors of that era systemically probed the skin to map out the area of lost sensation, a different story emerged. Most often the region of numbness corresponded not to the configuration of a dermatome but rather to the shape of various types of underwear of the period: corsets, drawers, bloomers, garters, stockings, and so on. This led many doctors of the time, including Sigmund Freud, to conclude that these numbing symptoms did not have a basis in damage to the sensory nerves, but that the perception of underwear-shaped numbness originated in the brain as a result of psychological and social factors. Today, underwear-shaped numbness is a much less common medical complaint. (It’s harder to imagine a numb thong-shaped region.)
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Touch»
Представляем Вашему вниманию похожие книги на «Touch» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Touch» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.