Richard J. Miron - Understanding Platelet-Rich Fibrin
Здесь есть возможность читать онлайн «Richard J. Miron - Understanding Platelet-Rich Fibrin» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Understanding Platelet-Rich Fibrin
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Understanding Platelet-Rich Fibrin: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Understanding Platelet-Rich Fibrin»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Understanding Platelet-Rich Fibrin — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Understanding Platelet-Rich Fibrin», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
In patients undergoing anticoagulant therapy, the simple addition of PRF during surgery can help favor faster clotting, thereby reducing bleeding times postoperative.
Platelets also release various GFs and cytokines that further lead to tissue regeneration but also attract macrophages and neutrophils to the defect site. These cells are responsible for clearing debris, replacing necrotic tissue, and removing bacteria from the wound site.
The proliferative phase begins by day 3, where the blood clot within the wound is further supplied with a provisional matrix typically composed in part with fibrin, which facilitates cell migration, while the clot within the vessel lumen contributes to hemostasis. 2Fibroblast cells are recruited to the wound site and begin producing new collagen in a random and somewhat disorganized order. Simulta-neously, new blood vessel formation leads to new angiogenesis, and the wound gradually begins to gain initial stability.
During the third and final stage (the remodeling phase), disorganized collagen is replaced by newly organized collagen fibrils that provide enhanced stability and strength to the injured site, where tissue regeneration takes place 4(see Fig 2-1).
Whole blood is comprised of four main components: blood plasma, red blood cells (RBCs), white blood cells (WBC), and platelets. Initially, platelets were reported as the major responsible component for the activation and release of crucial GFs for wound healing, including PDGF, coagulation factors, adhesion molecules, cytokines, and angiogenic factors. Their role has been extremely well described in the literature, so typically the entire field has been referred to as platelet concentrates or platelet-rich plasma/fibrin . Interestingly, however, over the years more attention has been placed on leukocytes, which are not only responsible for host defense but also highly implicated in the wound healing and regenerative phases.
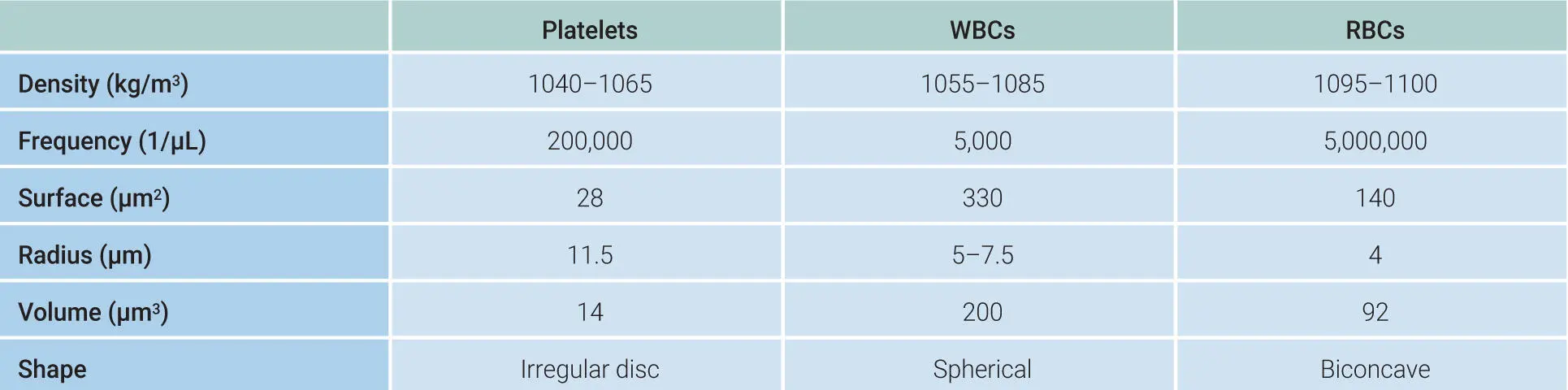
Table 2-1highlights the various cell types found in blood, including their density, frequency, and surface area. Note that while platelets are the lightest of the group, WBCs and RBCs are very similar in density. For these reasons they are also harder to separate in a centrifuge based on density. Noteworthy is the fact that per µL, there are 5,000,000 RBCs when compared to only 5,000 WBCs. Therefore, RBCs outnumber WBCs in a 1,000:1 ratio, which make them difficult to separate, especially on a fixed-angle centrifugation device as discussed later in this chapter ( Video 2-2).
Table 2-1Properties of cells found in whole blood

 Video 2-2
Video 2-2
Leukocytes and RBCs are similar in density. This makes these two cell types extremely difficult to separate, especially because RBCs outnumber them 1,000 to 1.
Cells in PRF
As shown in Table 2-1, the three main cell types found in PRP and PRF are platelets, leukocytes (WBCs), and RBCs. The entire initial goal of platelet concentrates was of course to concentrate platelets. Because they are the lightest of all cells found in blood, it was possible to utilize a centrifugation device to separate these layers based on their density. Lighter cells (platelets) could therefore be accumulated to the top, followed by leukocytes. Because RBCs are the densest of the group, they tend to migrate downward during the centrifugation process. In an ideal situation, the final PRF matrix should be composed of a high concentration of platelets, leukocytes, and fibrin. It has been shown that the initially developed PRF (also termed L-PRF for leukocyte PRF ) concentrates contained greater than 90% platelets and more than 50% leukocytes within a high-density fibrin network when compared to whole blood. 5By utilizing more advanced quantification devices and recently developed methods, our research team has been better able to harvest leukocytes specifically. The lower yield of leukocytes is typically a result of their more similar density to RBCs, making them harder to separate from and accumulate in the upper layers where PRF is collected. This is particularly difficult on fixed-angle centrifuges. Several other methods have been proposed to favor accumulation of cells, including shorter centrifugation times as well as lower centrifugation forces, as discussed later in this chapter (see section on the low-speed centri-fugation concept). 6
Leukocytes have been shown to be an integral component of PRF therapy and play a prominent role in wound healing. Studies from basic sciences and animal research have revealed how impactful a role leukocytes play during tissue regeneration by comparing PRP/PRF therapy with and without WBCs. 7–9In these split design studies, the contralateral side receiving leukocytes performed significantly better, promoting researchers and clinicians to develop protocols to better incorporate or harvest leukocytes. Naturally, PRF contains a higher number of leukocytes when compared to the first-generation platelet concentrates PRP and PRGF.
While the role of leukocytes has been well described as host defense against incoming pathogens, they also play a central role in immune modulation of biomaterials and participate in the wound healing process due to their ability to secrete key immune cytokines such as IL-1β, IL-6, IL-4, and TNF-α. 2,10,11They have been highly investigated in PRF therapy, with the impact of centrifugation speed and time affecting both their concentration and location, mainly owing to the fact that they are very similar in density and size to RBCs. Previously, it was demonstrated how faster protocols initially utilized to produce L-PRF were far too high in both g-force and time (2700 rpm for 12 minutes; ~700g). 6This led to the histologic observation that the majority of cells were concentrated either at the buffy coat region or at the bottom of centrifugation tubes within the RBC layer component. 6Based on these observations, it became clear that centrifugation speeds (g-forces) were evidently too high, pushing leukocytes especially down to the bottom of centrifugation tubes and away from the PRF clot. In order to redistribute leukocyte cell numbers across the entire PRF matrix, both a change in centrifugation speed and/or time (lower) as well as a change in the centrifugation device (horizontal centrifugation as opposed to fixed-angle) were deemed necessary to further improve platelet formulations, as reviewed later in this chapter.
Advantages of a 3D Fibrin Network
Fibrin is the activated form of a plasmatic molecule called fibrinogen that converts into fibrin with thrombin. Fibrin formation is one of the first key components to tissue wound healing. When an individual cuts himself, the first event taking place prior to any regeneration is fibrin clot formation. This is why patients on anticoagulant therapy typically do not heal quite as effectively because delayed clotting leads to delayed healing. The obvious advantage of PRF therapy is its ability to accumulate various cell types including platelets without anticoagulants, thereby improving clotting properties. Once a fibrin clot is formed during the centrifugation cycle, cells and GFs are able to be trapped within the 3D fibrin matrix, favoring the slower and gradual release of GFs from PRF over time. 12Fibrin is a soluble fibrillary molecule that is present in high quantity both in plasma itself as well as in the α-granules of platelets. Fibrin therefore plays a determining role in platelet aggregation during hemostasis and is critical to healing. Not surprisingly, the use of fibrin alone (without GFs or living cells as a fibrin glue) has been shown to lead to matrix stabilization favoring tissue stability, cellular invasion, and ultimately tissue regeneration. 13–15However, PRF has numerous advantages in that during the fibrin clot formation, a supraphysiologic concentration of platelets, leukocytes, and GFs are also present, forming a sort of “superclot” consisting of an intimate assembly of cytokines, glycanic chains, and structural glycoproteins enmeshed within a slowly polymerized fibrin network 16,17( Fig 2-2).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Understanding Platelet-Rich Fibrin»
Представляем Вашему вниманию похожие книги на «Understanding Platelet-Rich Fibrin» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Understanding Platelet-Rich Fibrin» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.