Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
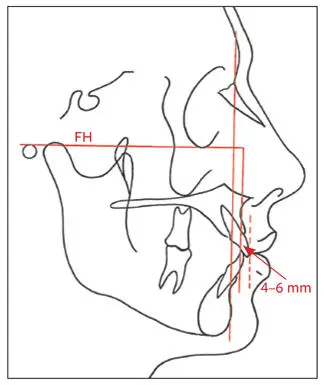
Fig 2-63Maxillary incisor position (McNamara). The labial surface of the incisor should be 4 to 6 mm ahead of the vertical line through A-point.
McNamara analysis. An important relationship, especially in orthognathic patients, is that of the incisors to the underlying basal bone of each jaw. In the McNamara analysis, the position of the maxillary incisors to their respective bone bases is determined by drawing a vertical line through A-point parallel to N and perpendicular to FH. The facial surface of the maxillary incisor should be 4 to 6 mm ahead of the line (Fig 2-63).
In maxillary dental protrusion cases, the incisor will be more than 6 mm ahead of the vertical line through A-point and will be an indication for orthodontic retraction. Where the maxillary incisors are upright (eg, in Class II, division 2 malocclusions), the incisor tip will be less than 4 mm ahead of this line or may be even behind it.
Mandibular incisor evaluation
Mandibular incisor position
Steiner analysis. The relative location of the mandibular incisors is determined by its relation to the N-B line (Fig 2-64). According to the Steiner analysis, the mandibular incisor angulation to the N-B line should be 25 degrees, and the most labial portion of the tooth crown should be 4 mm anterior to the line. However, the N-B line often is not reliable to assess the mandibular incisor position in patients with dentofacial deformities because of a lack of harmony between the mandible and the cranial base.
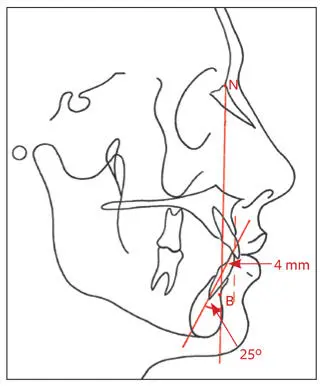
Fig 2-64Mandibular incisor position (Steiner): 25 degrees to N-B line, and 4 mm ahead of N-B.
The angular and linear measurements give an indication of the relationship of the mandibular incisors to the mandible. In individuals with Class III malocclusions and compensated incisors, the angle will be smaller and the incisor tip closer to the N-B line or even behind it. Protrusive incisors would produce a larger angle, and the labial surface would be more than 4 mm ahead of N-B. These measurements can also serve as a guide in planning for extractions and preoperative orthodontic positioning of the mandibular incisors.
McNamara analysis. As in the maxilla, in the mandible, it is important to determine the relationship of the mandibular incisors to the mandibular bony base. According to the McNamara analysis, the labial surface of the mandibular incisors should be 4 mm ahead of a true vertical line drawn through the B-point and at an angle of 25 degrees to the line (Fig 2-65a).
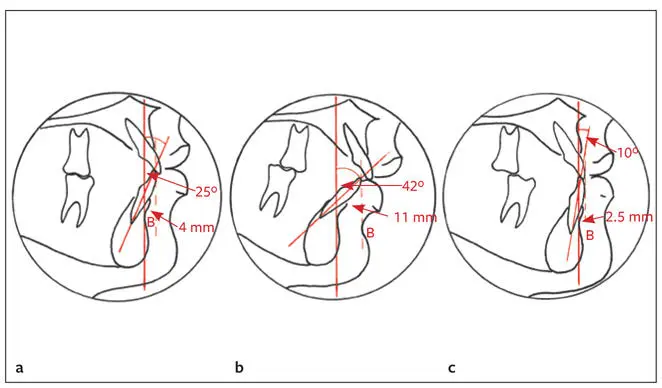
Fig 2-65 (a) Class I occlusion; incisor to vertical line through B-point: 4 mm and 25 degrees. (b) Class II malocclusion with mandibular incisor protrusion; incisor to vertical line through B-point: 11 mm and 42 degrees. (c) Class III malocclusion with compensated mandibular incisors; incisor to vertical line through B-point: 2.5 mm and 10 degrees.
An increase in this measurement indicates mandibular dental protrusion. In some racial groups, this measurement may be normal, but in Caucasians, it is often seen in Class II malocclusion with mandibular skeletal deficiency (Fig 2-65b). In Class III dental and skeletal relationships, the mandibular incisors are often compensated and are closer to this line or even behind it (Fig 2-65c).
Downs analysis. According to the Downs analysis, the ideal inclination of the long axis of the mandibular incisors to the mandibular plane is 90 ± 7 degrees (Fig 2-66). In individuals with Class III malocclusion and compensated mandibular incisors, this angle tends to be small. It tends to be larger when the lower incisors are protrusive (eg, in bimaxillary protrusion or Class II, division 1 malocclusion).
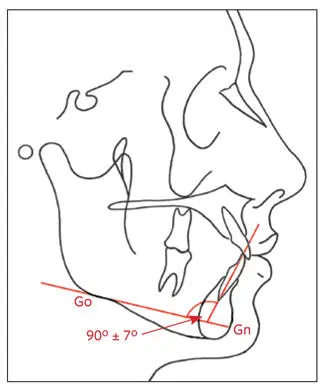
Fig 2-66Mandibular incisor position (Downs). The axial inclination of the mandibular incisor to the mandibular plane (Go-Gn) is 90 ± 7 degrees.
Interincisal angle (Downs)
The interincisal angle is formed by a line through the incisal edge and the apex of the root of the maxillary and mandibular central incisors (130 ± 6 degrees; Fig 2-67). The more protrusive the incisors, the smaller the angle. Low angles indicate protrusion of the incisors and are often associated with Class II, division 1 malocclusions. High angles are frequently associated with Class II, division 2 deep bites.
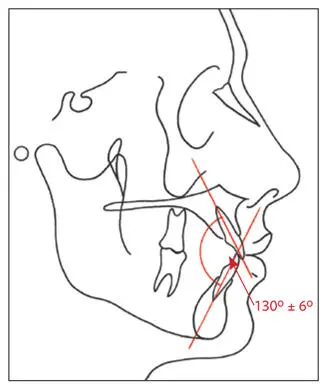
Fig 2-67Interincisal angle.
Maxillary molar to pterygoid vertical (Ricketts)
The distance from the pterygoid vertical (back of the maxilla) to the distal surface of the maxillary first molar (Fig 2-68) should be equal to the patient’s age + 3 mm. The distance will increase as the maxilla grows forward. For example, a 12-year-old child has a normal distance of 15 mm; an 18 year-old adult, 21 mm. It stabilizes at 24 mm in the adult, around age 21. This measurement helps determine whether a malocclusion is due to the maxillary or mandibular molar position. It is also useful in deciding whether extractions or headgear may be indicated and is indicative of the anteroposterior position of the maxilla. A small value indicates that the molar is too far distal, and thus headgear and distalization should be avoided; large values indicate the opposite. This measurement is influenced by previous maxillary tooth extractions allowing mesial drifting of the molar.
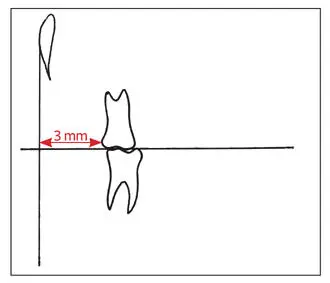
Fig 2-68Maxillary molar position. The distance from Ptv to the first molar should be the patient’s age + 3 mm.
Mandibular anterior dental height
The mandibular anterior dental height is measured from the mandibular incisor tip to the inferior border of the mandible. The average mandibular dental height is 44 ± 2 mm for males and 40 ± 2 mm for females (Fig 2-69). An increase in the mandibular vertical height of the face of a patient with normal upper lip length and normal maxillary incisor exposure may be caused by the anterior vertical height of the mandible. In this patient, vertical reduction genioplasty may be indicated.
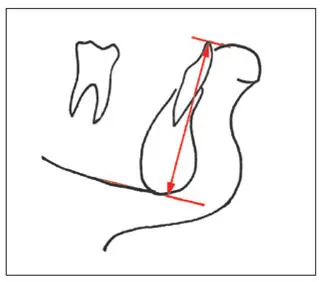
Fig 2-69Mandibular anterior dental height: 44 ± 2 mm for male patients and 40 ± 2 mm for female patients.
Occlusal plane angle
According to the Steiner analysis, the occlusal plane angle is formed between a line drawn through the region of the overlapping cusps of the first premolar and first molar bisecting the incisal overbite (the occlusal plane [OP]) and the anterior cranial base (S-N). The mean angle is 14 degrees (Fig 2-70). According to the Downs analysis, the angle is measured between the occlusal plane and the FH plane and should be 9 degrees.
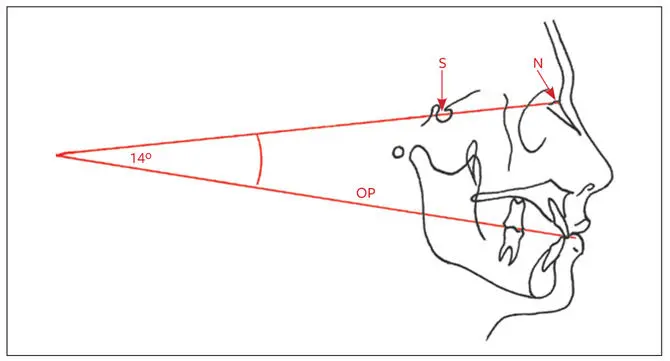
Fig 2-70Occlusal plane angle. Angle between OP and anterior cranial base (S-N).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.