Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Vertical and transverse dentoalveolar assessment
The vertical relationship between the basal bones and the dental and alveolar structures is evaluated by dropping perpendicular lines from the J-plane at YR and YL to the occlusal plane and from the S-plane to the occlusal plane at ZR and ZL. Transverse discrepancies are assessed by measuring the distances both from YR and YL and from ZR and ZL to the GM line. Vertical discrepancies are assessed by measuring the vertical heights from the J-plane to the occlusal plane, comparing left and right side heights. Mandibular dentoalveolar vertical discrepancies can be examined by measuring the vertical heights from the occlusal plane to the S-plane at ZR and ZL (Fig 2-75).
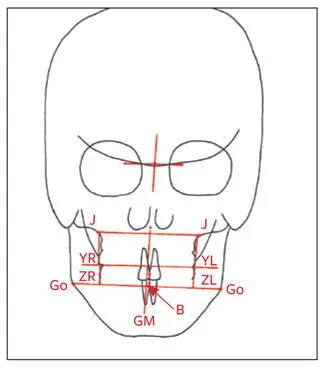
Fig 2-75Vertical dentoalveolar assessment.
The posteroanterior cephalometric analysis is helpful in assessing facial asymmetry. Also, in combination with the lateral cephalometric analysis, it gives the clinician a better dimensional understanding of dentofacial deformities. The lateral and posteroanterior cephalometric analyses of an individual with severe facial asymmetry involving the maxilla, mandible, and chin are demonstrated in Fig 2-76.
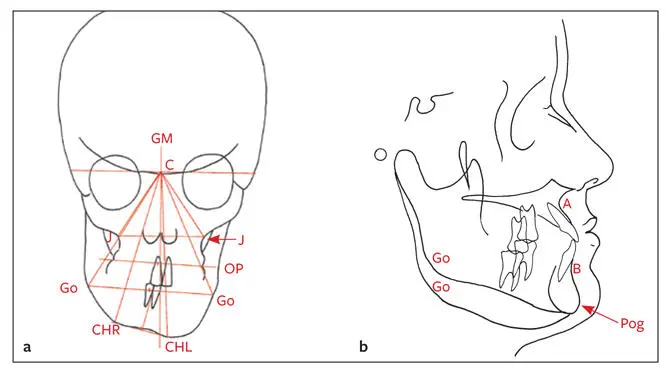
Fig 2-76 (a) Severe facial asymmetry. Note the severe rotation of the triangles. (b) The severe asymmetry is also evident on the lateral cephalometric tracing. The 3D nature of the facial asymmetry, a common finding in such cases, is well demonstrated.
Limitations of Cephalometric Analysis
Although cephalometric analysis is important in both diagnosis and development of a treatment plan, it has the following limitations:
Most individuals with dentofacial deformities have anatomical variations in the location of the cephalometric landmarks used as a baseline in many analyses, such as S, N, and Or. These anatomical variations often lead to incorrect conclusions from the analysis.
The clinician must not base interpretations on single cephalometric measurements.
The clinician must recognize the limitations as well as the advantages of cephalometry and be sure to integrate measurements with clinical findings.
The art of cephalometric interpretation lies in understanding abnormal findings and identifying the etiologic factors behind these cephalometric abnormalities in patients with dentoskeletal deformities.
Although cephalometric analysis forms an important part of the database for diagnosis and treatment planning, it should not take precedence over the clinical evaluation of the patient.
Full-Mouth Periapical Radiographic Evaluation
If a patient has any indication of periapical or periodontal pathology and/or dental caries, periapical radiographs should be taken to obtain a more detailed understanding of the pathologic condition. Periapical radiography can also more accurately assess the deviation of roots in areas of intended interdental osteotomies.
Panoramic Radiographic Evaluation
Panoramic radiography is an excellent means to establish an overview of the paranasal sinuses, bony temporomandibular joint (TMJ), periapical and periodontal pathology, dental caries, position of the inferior alveolar canal, position of the lingula, position of the mental foramen, tooth root lengths in relation to the maxillary sinus, and mandibular symphysis. Any suggestion of temporomandibular pathology should be further investigated by more specific radiographic examination. In addition, the panoramic radiograph can detect root deviations in areas of intended interdental osteotomies (although not as accurately as can a periapical radiograph), unerupted and/or impacted teeth, and previously undetected pathologic conditions. The information obtained is valuable not only in the pretreatment assessment but also in the determination of the relative position of anatomical structures, which is important during the actual surgical procedure. Figure 2-77 shows a panoramic radiographic evaluation form. It is essential that an immediate preoperative panoramic radiograph is available at the time of surgery because it gives the surgeon a valuable overview of anatomical structures relevant in most orthognathic surgical procedures (eg, position of the inferior alveolar canal, mental foramen, tooth roots, impacted third molars [if present], and maxillary sinuses).
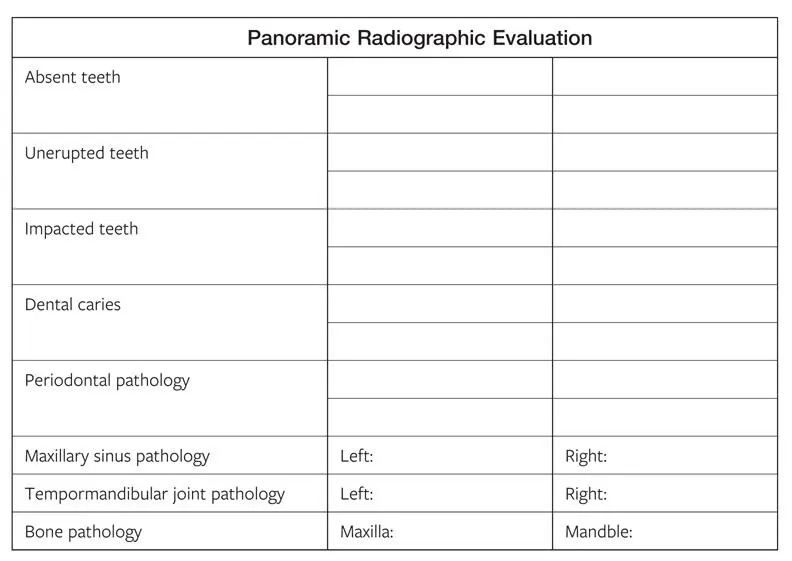
Fig 2-77Panoramic radiographic evaluation form. This evaluation should be used during the pretreatment assessment, at the presurgical examination, and at the time of surgery.
Occlusion and Study Cast Evaluation
Occlusal functional evaluation
The basic aims of occlusal functional evaluation are to determine the compatibility of centric occlusion (CO) and centric relation (CR); to note the difference between CO and CR, if present; to note any bite of convenience or occlusal slide; and to note interocclusal rest space. Figure 2-78 is a sample functional evaluation form.
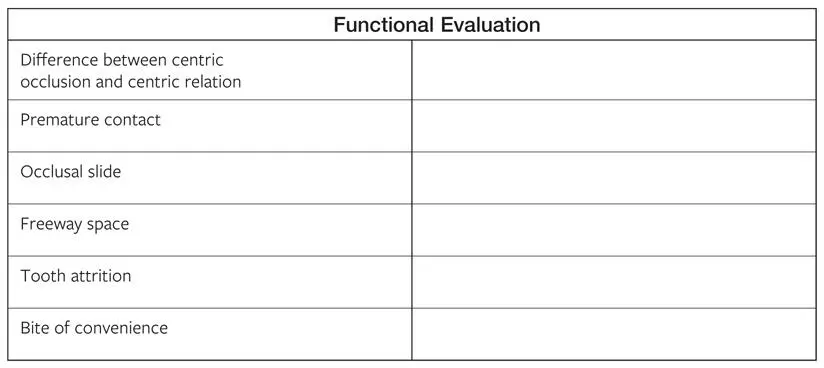
Fig 2-78Functional evaluation form.
Study cast analysis
Intra-arch relationship
In the study cast analysis, arch form and symmetry, missing teeth, tooth rotations, and overerupted teeth are noted. Maxillary and mandibular occlusal curves are studied. Crowding and the need for extractions are determined. Bolton discrepancies of tooth sizes are studied. Any tooth size discrepancies should be noted and compensated for during the preoperative orthodontic treatment stage. Tooth size discrepancy influences arch compatibility and leads to poor occlusal fit at surgery.
Interarch relationship
The study cast analysis also includes examination for incisor overjet and overbite, as well as Angle classification for molars and canines. The clinician evaluates coordination of dental midlines and crossbites while moving the dental casts into a Class I malocclusion to get an idea of general arch compatibility.
If the possibility of establishing an acceptable occlusion, accommodating the teeth, or providing for tooth size discrepancies is at all questionable, a Kesling diagnostic setup should be used. This setup also can be used to test for various extraction patterns.
If a crossbite exists with the teeth in CO and it is corrected when the dental casts are moved into a Class I occlusion, the crossbite is considered relative. If the crossbite still exists after the dental casts have been positioned in a Class I relationship, the crossbite is considered absolute (see chapter 5, Fig 5-38).
A sample form for study cast analysis is presented in Fig 2-79.
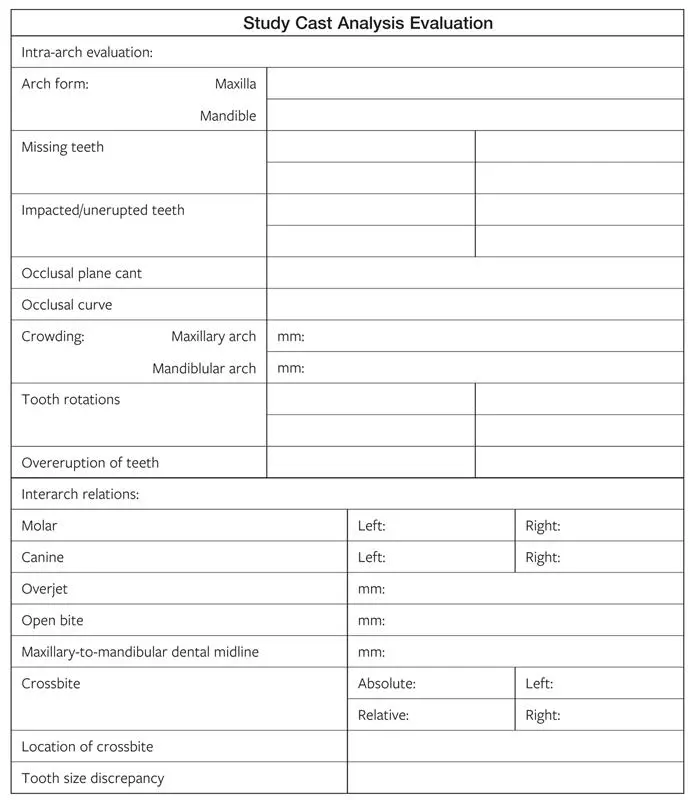
Fig 2-79Study cast analysis form.
TMJ Evaluation
The TMJ is an important component of the orthognathic mechanism and should be examined with care. Pathologic conditions may be present in the joint at the outset, may develop during treatment, or may even develop long after treatment. Therefore, the clinician should diagnostically and prognostically evaluate the joint before orthodontic-surgical treatment begins. A basic TMJ examination evaluates three areas: (1) mandibular movements, (2) TMJ signs and symptoms, and (3) mouth opening and deviations.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.