Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
SNA angle (Steiner)
The SNA angle is formed between the anterior cranial base (S-N) and a line drawn through N and A-point. Its mean is 82 degrees (Fig 2-52). The SNA angle gives an indication of the anteroposterior position of the maxilla relative to the anterior cranial base. An angle less than 82 degrees is indicative of maxillary anteroposterior deficiency, whereas an increased angle may indicate maxillary protrusion.
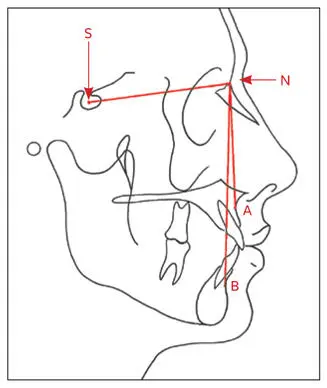
Fig 2-52Steiner analysis for maxillary and mandibular anteroposterior positions relative to the anterior cranial base (S-N). SNA is 82 degrees. SNB is 80 degrees. The maxillomandibular relationship is indicated by the ANB angle (mean, 2 degrees).
SNB angle (Steiner)
The SNB angle is formed between the anterior cranial base (S-N) and a line drawn through N and B-point. Its mean is 80 degrees (see Fig 2-52). The angle gives an indication of the anteroposterior position of the mandible relative to the anterior cranial base. Patients with mandibular anteroposterior excess will have an angle greater than 80 degrees. Those with mandibular deficiency will have a decreased angle.
ANB angle (Steiner)
The ANB angle is formed between A-N and N-B. Its mean is 2 degrees (see Fig 2-52). The angle provides an idea of the anteroposterior discrepancy between the maxilla and the mandible. In Class III cases, the angle is less than 2 degrees or even negative; in Class II cases, the angle is increased.
In spite of its shortcomings, Steiner analysis continues to be a popular method of evaluating the anteroposterior relationship of the maxilla and mandible. However, this analysis should not be used to make an absolute diagnosis of sagittal skeletal disharmony because vertical and rotational jaw dimensions relative to the anterior cranial base often have a significant effect on the measurements (see the next section).
Wits appraisal
Most cephalometric analyses, like Steiner analysis, relate the maxillary and mandibular anteroposterior position to the cranium. Measurements from the cranial base, however, do not always provide a reliable expression of the anteroposterior relationship between the maxilla and mandible. The Wits appraisal is a linear measurement between the maxilla and mandible and is not influenced by the cranium.
Points BO and AO are established by dropping perpendicular lines from the A-point and B-point, respectively, onto the occlusal plane (Fig 2-53). The mean in males is BO 1 mm ahead of AO. In females, BO and AO coincide. The measurement between BO and AO indicates the anteroposterior discrepancy between the maxilla and the mandible. A small discrepancy may indicate that a patient can be treated orthodontically, whereas a large discrepancy may indicate that surgical correction will be required.
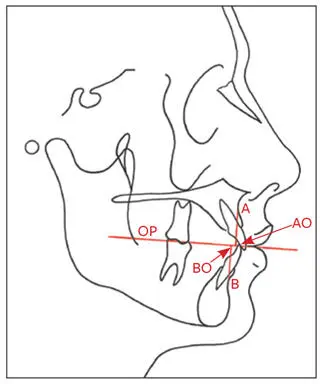
Fig 2-53Wits appraisal. Vertical lines are drawn perpendicular to the occlusal plane (OP) from A-point and B-point. The points of contact on the OP are labeled AO and BO, respectively.
Clockwise or counterclockwise rotations of the maxillomandibular complex relative to the anterior cranial base do not affect the Wits appraisal measurements. However, these rotations significantly affect Steiner analysis. This is a good example of how two cephalometric analyses may render quite contradictory measurements; however, the observations assist in treatment planning. Figures 2-54a to 2-54c illustrate three cases with the same Wits measurements (0 mm) but ANB angles of +2, +8, and –2 degrees and very different facial profiles. Surgical rotation of the maxillomandibular complex may be indicated for correction in the cases depicted in Figs 2-54b and 2-54c. The case in Fig 2-54d has an ANB angle of –1 degree, indicating a mild Class III discrepancy between the jaws. The Wits appraisal for this case, however, is 8 mm, indicating a substantial jaw discrepancy; the patient could not be treated by orthodontic means alone.
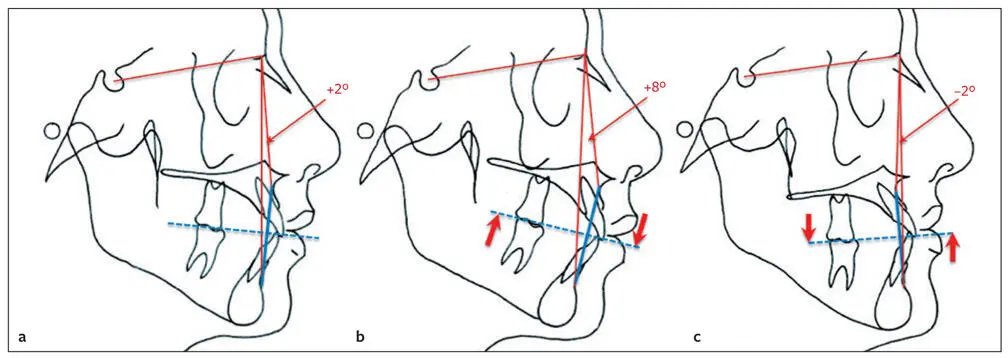
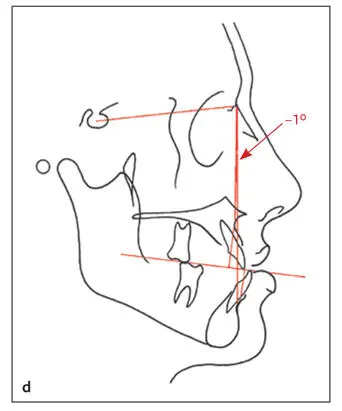
Fig 2-54The effect of rotation of the maxillomandibular complex relative to the anterior cranial base and the ANB angle. (a) Normal relation: ANB angle is +2 degrees. (b) Counterclockwise rotation resulting in an ANB angle of +8 degrees. (c) Clockwise rotation with an ANB angle of –2 degrees. In all three cases, the Wits appraisal (blue line) indicates a normal relationship (0 mm) between the maxilla and mandible. (d) An ANB angle of –1 degree indicates a mild Class III jaw relationship (Steiner). According to the Wits appraisal, the discrepancy between the maxilla and mandible is severe (8 mm).
Facial angle (Downs)
The facial angle is the inferior inside angle in which the facial line (N-Pog′) intersects the FH. Its mean is 82 to 95 degrees (Fig 2-55). The facial angle indicates the relative anteroposterior position of the mandible to the cranium.
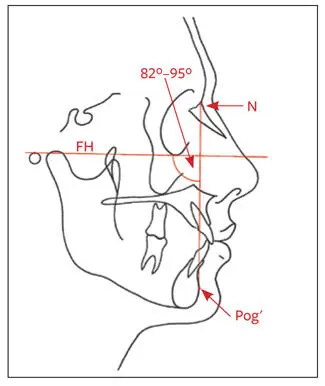
Fig 2-55Facial angle. The mean is 82 to 95 degrees.
Maxillary depth (McNamara)
The maxillary depth is the horizontal distance between N and A-point. It is calculated by drawing a line through N perpendicular to FH until A-point is reached (Fig 2-56). Its mean is 0 mm. A-point is expressed as a positive value anterior to the line and as a negative value posterior to the line. The maxillary depth is an indication of the anteroposterior position of the maxilla in relation to the cranium.
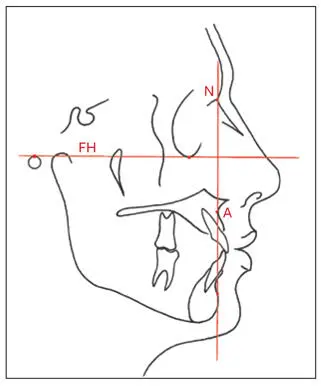
Fig 2-56Maxillary depth. A line is drawn through N perpendicular to FH. A-point (maxillary position) is expressed as positive anterior to the line and as negative posterior to the line.
Anteroposterior and vertical relationships (McNamara)
The lower anterior facial height is measured from ANS to Me, and the midfacial length is measured from Co to A-point. The distance from Co to Gn constitutes the mandibular length (Fig 2-57). There should be a correlation between the lower anterior facial height (ANS-Me), the length of the midface (Co-A), and the mandibular length (Co-Gn). The correlations are listed in Table 2-11.
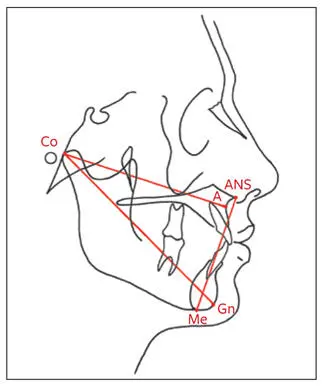
Fig 2-57Lower anterior facial height: ANS-Me. Midfacial length: Co-A. Mandibular length: Co-Gn.
Table 2-11| Normative standards (mm) in McNamara analysis
| Midfacial length (Co-A) | Mandibular length (Co–Gn) | Lower anterior facial height (ANS–Me) |
| 80 | 97–100 | 57–58 |
| 81 | 99–102 | 57–58 |
| 82 | 101–104 | 58–59 |
| 83 | 103–106 | 58–59 |
| 84 | 104–107 | 59–60 |
| 85 | 105–108 | 60–62 |
| 86 | 107–110 | 60–62 |
| 87 | 109–112 | 61–63 |
| 88 | 111–114 | 61–63 |
| 89 | 112–115 | 62–64 |
| 90 | 113–116 | 63–64 |
| 91 | 115–118 | 63–64 |
| 92 | 117–120 | 64–65 |
| 93 | 119–122 | 65–66 |
| 94 | 121–124 | 66–67 |
| 95 | 122–125 | 67–69 |
| 96 | 124–127 | 67–69 |
| 97 | 126–129 | 68–70 |
| 98 | 128–131 | 68–70 |
| 99 | 129–132 | 69–71 |
| 100 | 130–133 | 70–74 |
| 101 | 132–135 | 71–75 |
| 102 | 134–137 | 72–76 |
| 103 | 136–139 | 73–77 |
| 104 | 137–140 | 74–78 |
| 105 | 138–141 | 75–79 |
Maxillary-mandibular anteroposterior relationship (McNamara)
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.