Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
When the patient’s lips are relaxed, 1 to 4 mm of the maxillary incisors should be visible under the upper lip. Lack of tooth exposure may be an indication of maxillary vertical deficiency; more than 4 mm of tooth exposure may indicate vertical maxillary excess (see Fig 2-37). The upper lip length should be kept in mind with this assessment.
Patients with relatively normal upper lips and excessive incisor exposure under the upper lip will have vertical maxillary excess. This assessment can be made only with the lips in repose. Lack of tooth exposure under an upper lip of normal length is an indication that the maxilla is vertically deficient. Vertical maxillary deficiency can be assessed only with the bite opened until the lips begin to part.
Upper and lower lip vermilion height
The upper lip vermilion height should be 25% less than the lower lip vermilion height. In short, the ratio of Ls-Sts to Sti-Li should be 3:4 (see Fig 2-37). Vermilion heights may vary depending on race, a fact that should be kept in mind during evaluation. Increased lower lip vermilion exposure may be due to lower lip eversion caused by lip incompetence in patients with vertical maxillary excess. The lower lip is also often everted in Class II deep bite cases or Class II, division 1 cases where the lower lip is rolled outward by the maxillary incisors.
Table 2-8summarizes the vertical soft tissue relationships.
Table 2-8| Summary of vertical soft tissue relationships
| Vertical relationship | Measurement | Normal value |
| Middle facial height: lower facial height (MFH:LFH) | G'-Sn:Sn–Me' | 1:1 |
| Upper lip length (ULL) | Sn–Sts | 20 ± 2 mm (females) 22 ± 2 mm (males) |
| Lower lip/chin length (LLL) | Sti–Me' | 40 ± 2 mm (females) 44 ± 2 mm (males) |
| Upper lip length: lower lip/chin length (ULL:LLL) | Sn–Sts:Sti–Me' Sn–LLV:LLV–Me' | 1:2 1:0.9 |
| Interlabial gap (ILG) | NA | 0 to 3 mm |
| Maxillary incisor tooth exposure (ITE) | Sts–Maxillary incisor tip | 1 to 4 mm |
| Upper lip vermilion:lower lip vermilion (ULV:LLV) | Ls–Sts:Sti–Li | 3:4 |
NA, not applicable.
Soft tissue anteroposterior evaluation
Nasolabial angle
The nasolabial angle is formed by a line tangent to the columella and a line tangent to the upper lip. A value of 85 to 105 degrees is considered normal. In males, the angle is usually more acute, whereas in females, a more obtuse angle is considered to be attractive (Fig 2-38).
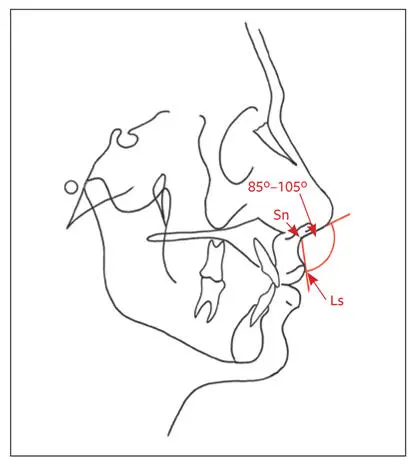
Fig 2-38The nasolabial angle is formed by a line tangent to the columella and a line tangent to the upper lip (Sn-Ls).
The nasolabial angle is influenced by the position of the upper lip supported by the maxillary incisors and the inclination of the columella of the nose. Excessive orthodontic retraction of the maxillary incisors will undermine upper lip support, leading to an unattractive increase of the nasolabial angle. The angle is more acute in Class III cases and more obtuse in Class II cases. The following factors that may influence the nasolabial angle should be considered during treatment planning:
Lip support. The existing maxillary incisor–upper lip relationship must be assessed.
Lip strain. Strained lips tend to move posteriorly once tension has been released. Tense lips, however, move less anteriorly with tooth or bone movement.
Lip thickness. Thin lips respond more readily than thick lips to tooth movement.
Magnitude of the overjet. If orthodontic retraction of maxillary incisors is contemplated, the larger the overjet, the more retraction that will be necessary. This retraction may lead to an increase in the nasolabial angle and loss of lip support.
The final anteroposterior position of the maxillary incisors and anteroposterior lip position are affected by interdental crowding or spaces in the anterior maxillary dental arch, tooth size discrepancies (maxillary versus mandibular), extraction versus nonextraction, extraction pattern (first versus second premolars), and existing tooth angulation.
Lip prominence
A line is drawn from Sn to Pog' (lower facial plane). The perpendicular distance of the Ls ahead of the Sn-Pog' line should be 3 ± 1 mm, whereas the Li should be 2 ± 1 mm anterior to the Sn-Pog' line (Fig 2-39a).
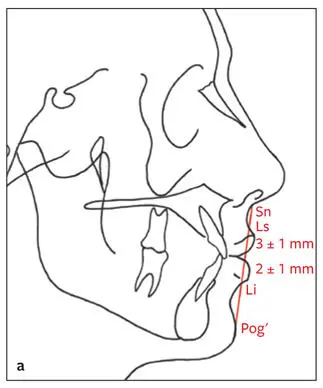
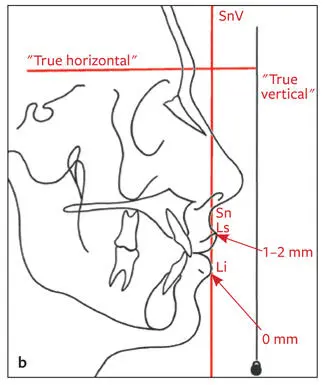
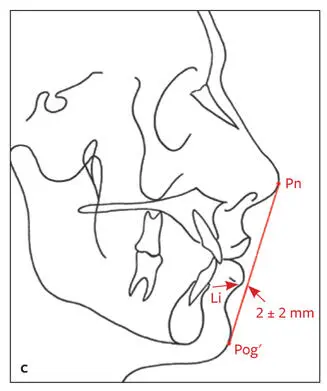
Fig 2-39 (a) Lip prominence in relation to the lower facial plane. The distance of Ls and Li to Sn-Pog′ is measured. Ls to Sn-Pog′: 3 ± 1 mm. Li to Sn-Pog′: 2 ± 1 mm. (b) Lip prominence in relation to SnV. The distances of Ls and Li are measured to the line drawn parallel to true vertical through the Sn. Ls to SnV: 1 to 2 mm. Li to SnV: 0 mm. (c) Lip prominence in relation to the E-line. Li should be 2 ± 2 mm behind Pn-Pog′.
The anteroposterior position of the upper lip is an indication of soft tissue support by the maxillary incisors and plays an important role in orthodontic or surgical positioning of the maxillary incisors. Thus, it should be kept in mind during treatment planning. The Li tends to be further ahead of Sn-Pog' in Class II cases (with Pog′ posteriorly situated) and behind the line in Class III cases (with Pog' anteriorly situated).
A vertical line drawn through the Sn perpendicular to “true horizontal” is called the subnasale vertical (SnV), and the upper lip should be 1 to 2 mm ahead of SnV. The lower lip should be on or just posterior to SnV (Fig 2-39b). In cases of mandibular anteroposterior deficiency, the lower lip tends to be more than 1 mm posterior to SnV. In patients with mandibular anteroposterior excess and/or maxillary anteroposterior deficiency, the lower lip will be anterior to the SnV. The distance of the most prominent part of the lower lip is measured to the E-line (Pn-Pog'). The lower lip should be 2 ± 2 mm behind the E-line (Fig 2-39c).
This evaluation is influenced by the nose and chin prominence and could also be used for planning the final chin position. The lower lip would tend to be ahead of this line in individuals with Class II mandibular anteroposterior deficiency, in whom Pog' is situated posteriorly and the lower lip everted.
Maxillary and mandibular anteroposterior position
A vertical line perpendicular to the constructed horizontal plane is drawn through G'. Pog' should be 1 to 4 mm behind the line. For maxillary anteroposterior assessment, Sn should be 6 ± 3 mm ahead of this line (Fig 2-40).
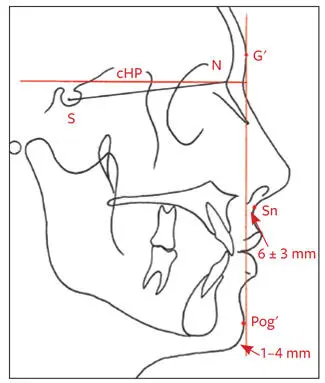
Fig 2-40Maxillary and mandibular anteroposterior position. Sn should be 6 ± 3 mm ahead of the vertical line drawn through G′, and Pog′ should be 1 to 4 mm behind this line.
In patients with maxillary anteroposterior deficiency, Sn will be less than 3 mm ahead of the line, or in severe cases, even behind the line. Pog′ ahead of the line indicates possible mandibular anteroposterior excess. In mandibular anteroposterior deficiency, Pog′ will be more than 4 mm behind the line. It is important, however, to evaluate the anteroposterior position of the chin in conjunction with other features (particularly the shape of the chin) to distinguish among microgenia, macrogenia, and mandibular anteroposterior deficiency.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.