Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
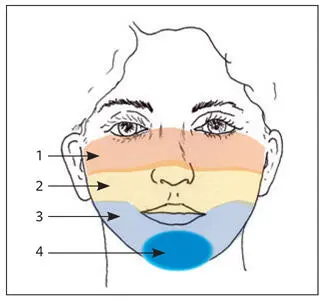
Fig 2-22The face can be divided into oculonasal (1), maxillary (2), and mandibular (3) complexes. The mandibular complex includes the genial subcomplex (4).
Profile analysis
Upper third of the face
The supraorbital rims normally project 5 to 10 mm beyond the most anterior projection of the globe of the eye. Frontal bossing, supraorbital hypoplasia, exophthalmos, or enophthalmos should be distinguished.
Middle third of the face
It is helpful to examine the middle and lower thirds of the face in isolation, and masking the lower third with a card eliminates any undue influence that this third may have on the perceptions of the face as a whole. The middle third of the face can also be blocked out to evaluate only the lower third in relation to the rest of the face (Fig 2-23). The nose, cheeks, and paranasal areas are sequentially evaluated.
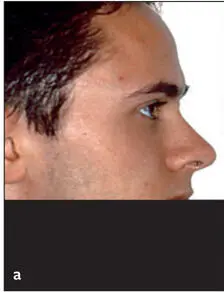
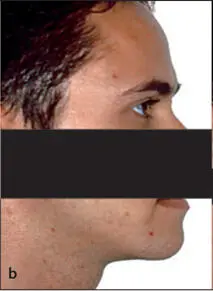

Fig 2-23 (a) The mandibular complex (including the chin) is blocked out, revealing the deficient paranasal flattening and poor upper lip support. (b) The middle third of the face is blocked out, showing the mandible and chin in good relation to the rest of the face. This observation is confirmed when only the upper lip and maxilla are blocked out (c) .
Nose
The shape of the dorsum is noted as normal, convex, or concave. The projection of the nasal bridge should be anterior to the globes (5 to 8 mm). The appearance of the nasal tip is evaluated for the presence of a supratip break and for tip definition and projection (Fig 2-24). It is important to distinguish between a dorsal hump and a turned-down tip because each has different treatment implications. The possible effect of maxillary surgery on the nose should be kept in mind when evaluating the proportions of the base of the nose (Fig 2-25).
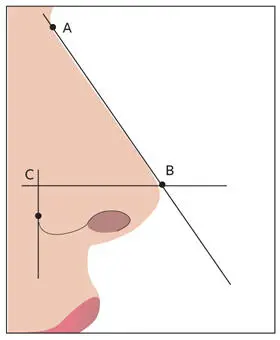
Fig 2-24The nasal tip projection is evaluated by the Goode method. If BC is greater than 55% to 60% of AB, the nasal tip usually appears disproportionately overprojected.
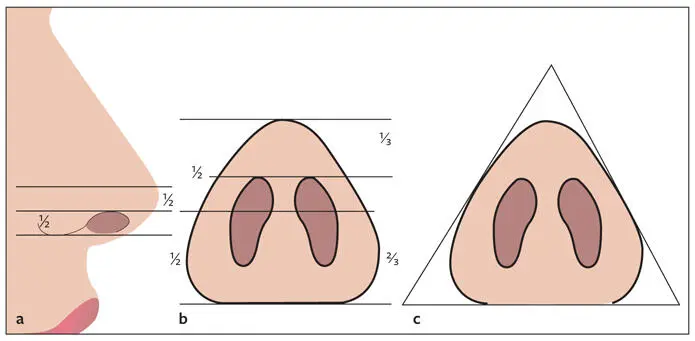
Fig 2-25 (a) Vertical ala–columella relationship. (b) Columella-lobule relationship with a ratio of approximately 2:1. (c) The general shape of the alar base should resemble an isosceles triangle, with the lobule neither too broad nor too narrow.
Cheeks
The globes generally project 0 to 2 mm ahead of the infraorbital rims, whereas the lateral orbital rims lie 8 to 12 mm behind the most anterior projection of the globes (Fig 2-26). The cheeks should exhibit a general convexity from the apex of the cheekbone to the commissure of the mouth. This line of convexity, called the cheekbone–nasal base–lip curve contour , requires simultaneous frontal and profile examination. This line starts just anterior to the ear, extending forward through the cheekbone, then antero-inferiorly over the maxilla adjacent to the alar base of the nose, and ending lateral to the commissure of the mouth (Fig 2-27). The line should form a smooth, continuing curve with no interruptions. An interruption of the curve may indicate an apparent skeletal deformity. Figure 2-28 illustrates a clear interruption of this line in the maxillary area, indicating maxillary anteroposterior deficiency. In Fig 2-29, the interruption in the line is in the maxillary area, indicating maxillary anteroposterior deficiency, and inferior to the upper lip section, indicating mandibular anteroposterior excess.
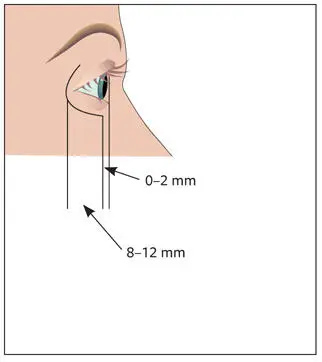
Fig 2-26The lateral orbital rim lies 8 to 12 mm behind the globe, and the globe projects 0 to 2 mm ahead of the infraorbital rim.
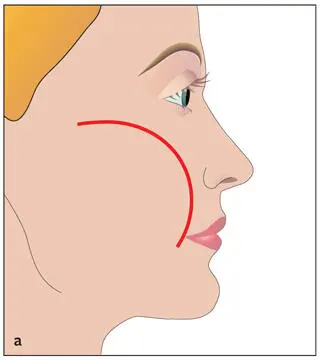
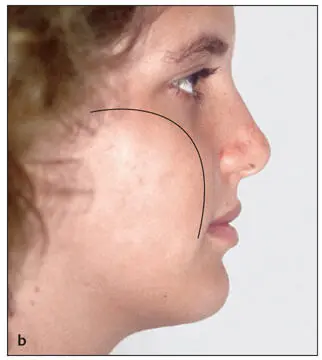
Fig 2-27 (a) Cheekbone–nasal base–lip curve contour. (b) Note the smooth, uninterrupted curve of the contour line in an individual with good facial proportions.
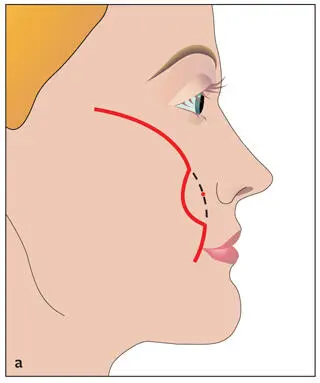
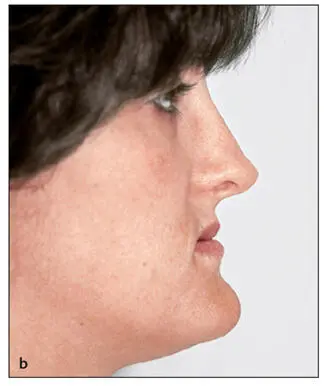
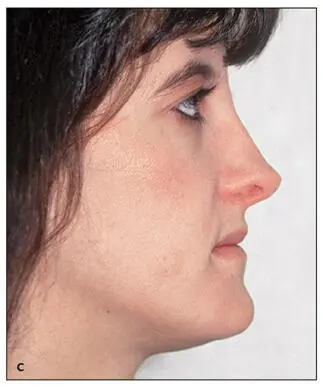
Fig 2-28 (a and b) An interruption in the curve of the contour line at MxP, indicating maxillary anteroposterior deficiency. (c) An improvement in the curve after advancement of the maxilla.
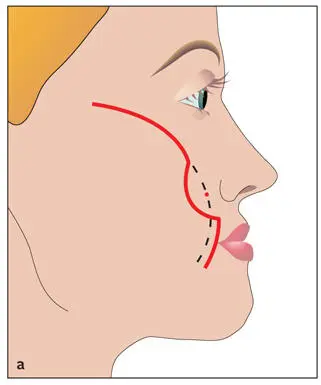
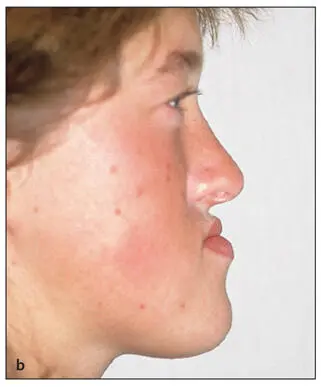
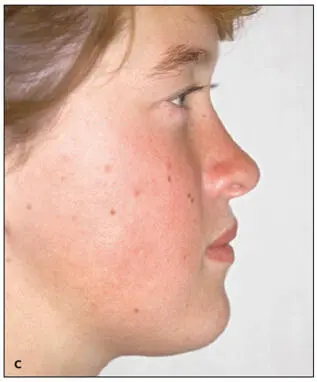
Fig 2-29 (a and b) A double break in the contour line in an individual with maxillary anteroposterior deficiency and mandibular anteroposterior excess. (c) The curve in the contour line is more harmonious after surgical advancement of the maxilla and mandibular setback.
Paranasal areas
The clinician should carefully assess the paranasal area because it plays an important role in distinguishing between middle third deficiency and mandibular anteroposterior excess. The ratio of the linear distance (horizontally) from nasal tip to Sn and from Sn to alar base crease is normally 2:1 (Fig 2-30). A ratio closer than 1:1 indicates maxillary anteroposterior deficiency. An increased ratio indicates decreased nasal projection. Patients with a Class III malocclusion, decreased nasal projection, and a short nose should be treated by mandibular setback rather than maxillary advancement. The possibility of rhinoplasty as a second procedure should be discussed with the patient.
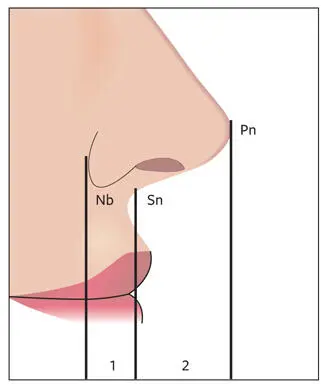
Fig 2-30Nasal projection. The projection of the nose is measured horizontally from Pn to Sn and is normally 16 to 20 mm. From the nasal base (Nb), the ratio of Pn-Sn to Sn-Nb should be 2:1.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.