Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Middle third of the face
The nose, center of the lips, and middle of the chin (in the lower third of the face) should fall along a true vertical line ( Table 2-2). Generally, no sclera is seen above or below the iris in a relaxed eyelid position with the patient looking straight ahead in natural head posture. Individuals with a midface deficiency tend to show sclera below the iris of the eye (Fig 2-14).
Table 2-2| Comparison of excessive and deficient midface dimensions
| Excessive middle third | Deficient middle third | |
| Vertical maxillary dimension | Excessive | Deficient |
| Cheeks | Sallow | Full |
| Sclera showing | Visible below the iris | Normal |
| Cheekbones | Flat | Prominent, broad |
| Paranasal areas | Flat | Full |
| Nose | Narrow, long | Short, broad |

Fig 2-14Sclera shows below the irises of the eyes in this individual with midface deficiency.
Sequential evaluation of the cheekbones, paranasal areas, alar eminences, and upper lip relation (in the lower third) should be performed. The cheekbone–nasal base–lip contour is a convenient contour line to evaluate the harmony of the structures of the midface (zygoma, maxilla, and nasal base) with the paranasal area and upper lip. This line starts just anterior to the ear, extends forward through the cheekbone, and then runs anteroinferiorly over the maxilla adjacent to the alar base of the nose, ending lateral to the commissure of the mouth. The line should form a smooth, continuing curve (Fig 2-15). An interruption of the curve may be an indication of an apparent skeletal deformity. Figure 2-16 illustrates a clear interruption of the line in the maxillary area, indicating maxillary anteroposterior deficiency. In Fig 2-17, there is a double break with one indicating maxillary deficiency and the other an interruption in the lower part because of mandibular anteroposterior excess.
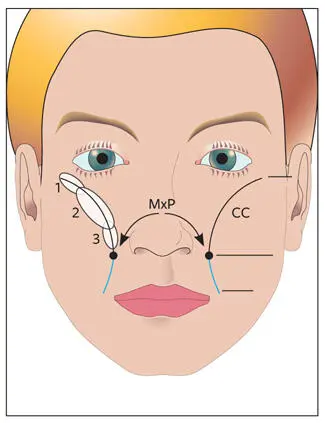
Fig 2-15Cheekbone–nasal base–lip contour. The cheekbone area (CC) is divided into three parts: (1) zygomatic arch, (2) middle area, and (3) subpupillary area. The maxillary point (MxP) is the most medial point on the curve. The nasal base–upper lip contour (blue) extends inferiorly from MxP. The line should curve gently, without interruptions, ending lateral to the corner of the mouth.
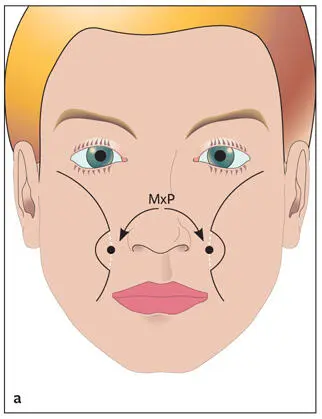
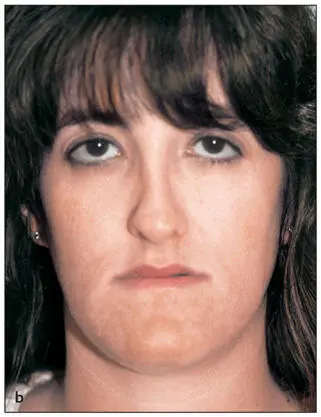
Fig 2-16 (a) Interruption of the curve at MxP. (b) Individual with maxillary anteroposterior deficiency. There is an interruption in the cheekbone–nasal base–lip contour at MxP.
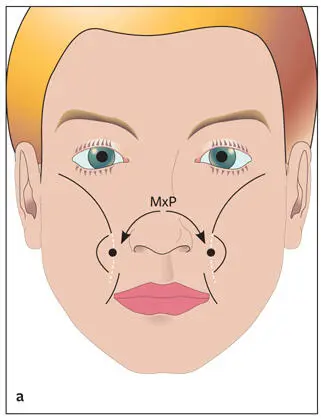
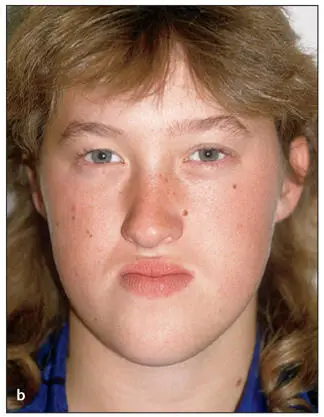
Fig 2-17 (a) Interruption of the curve at MxP and below MxP. (b) An individual with maxillary anteroposterior deficiency and mandibular prognathism. The cheekbone–nasal base–lip contour is interrupted with a double break, at MxP and also below MxP.
Lower third of the face
The middle third to lower third vertical height of the face should have a 5:6 ratio ( Table 2-3). The length from Sn to stomion superius (Sts; called the upper lip length ) should make up one-third of the lower third facial height. The distance from stomion inferius (Sti) to Me', the lower lip length , should equal two-thirds of the lower third face height (see Fig 2-13).
Table 2-3| Comparison of excessive and deficient lower face height
| Excessive lower third | Deficient lower third | |
| Vertical maxillary dimension | Excessive | Deficient |
| Lip appearance | Increased interlabial gap | Overclosed |
| Smile | Gummy | Toothless |
| Maxillary incisor exposure | Excessive | Little or none |
| Chin | Microgenia | Macrogenia |
| Malocclusion | Class II with or without anterior open bite | Class III closed bite or Class II deep bite |
Normal upper lip length is 20 ± 2 mm for females and 22 ± 2 mm for males, measured from Sn to upper lip inferior (Sts). If the upper lip is anatomically short, there is a tendency for the interlabial gap to be larger than normal and for increased maxillary tooth exposure with normal lower facial height. This condition should not be confused with skeletal vertical maxillary excess. The distance from lower lip superior (Sti) to Me' is 40 ± 2 mm for females and 44 ± 2 mm for males. The lower lip may often appear short because of posture caused by maxillary incisor interference in patients with deep bite. The upper lip length should be related to lower anterior dental height.
With the patient’s lips in repose, the amount of maxillary incisor exposure beneath the upper lip should be noted (Fig 2-18). For individuals in whom the maxillary incisors are not visible under the upper lip, the tooth-lip relation should be evaluated with the mandible rotated open until the lips just separate (Fig 2-19). The relation of the dental midline to the facial midline is an important aspect to note because dental midlines can be coordinated and/or corrected either orthodontically or surgically. The etiology of dental midline shifts may be dental or skeletal. Dental factors that may cause midline shifts include spaces; missing teeth; tooth rotations; malpositioned teeth; crowding; crowns, fixed partial dentures, fillings, or implants (which can all change the size of teeth); and tooth size discrepancy.
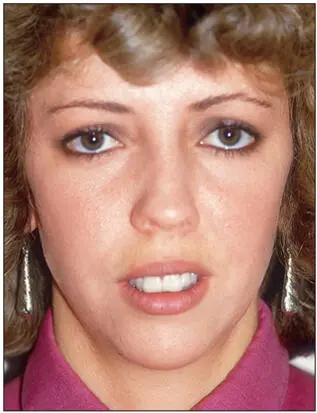
Fig 2-18Excessive maxillary incisor exposure and increased interlabial gap. Normal maxillary incisor exposure under the upper lip is 1 to 4 mm. This measurement will be influenced by upper lip length, vertical maxillary length, lip thickness, and the angle and anteroposterior position of the maxillary incisors.
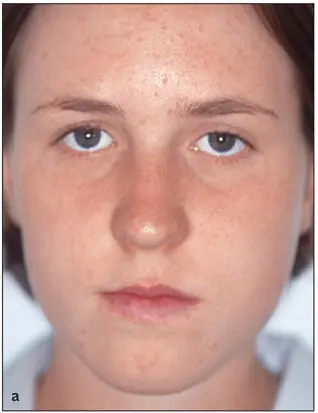
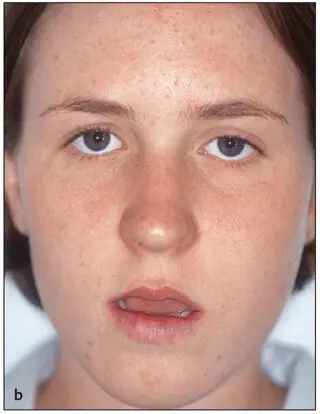
Fig 2-19Individual with vertical maxillary deficiency. (a) It is not possible to assess maxillary incisor–lip relationship with the teeth in occlusion. (b) The lack of maxillary incisor exposure is evident with the mandible rotated open until the lips part and the upper lip is relaxed and not influenced by the lower lip.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.