Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Lower third of the face
A systematic examination of the lower third of the face includes evaluation of the lips, labiomental fold, nasolabial angle, chin, and chin-throat area.
Lips
The protrusion, retrusion, and soft tissue thickness of each lip is evaluated with the lips in repose. The upper lip usually projects slightly anterior to the lower lip. The position of the lips relates to the underlying dental position, such as maxillary dental protrusion or lack of upper lip support caused by, for example, Class II, division 2 malocclusion or excessive orthodontic retraction of maxillary incisors. An individual with an excessive increase in lower lip vermilion and a deep labiomental fold often also has a Class II, division 1 malocclusion.
The anteroposterior lip position may be assessed with the help of the esthetic line of Ricketts (E-line) or esthetic plane of Steiner (S-line) as guidelines (see the following sections on cephalometrics). The Sn-Pog' line, also called the lower facial plane , is an important guide in assessing the lip position and planning orthodontic and surgical positioning of the incisors, as well as surgical positioning of the chin. The upper lip should be 3 ± 1 mm ahead of this line and the lower lip 2 ± 1 mm ahead of this line. Extractions followed by retraction of incisors behind the Sn-Pog' line should be avoided. Keep in mind that this assessment is influenced by the anteroposterior position of the chin and the soft tissue thickness of the lips (Fig 2-31).
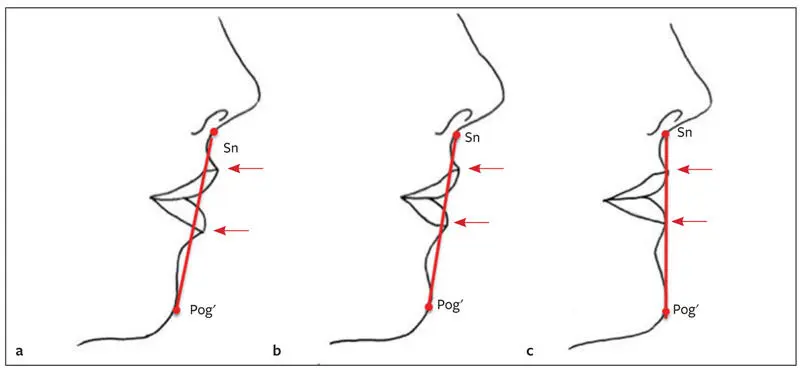
Fig 2-31Effect of the chin position on the Sn-Pog′ line. (a) Effect in an individual with mandibular anteroposterior deficiency (lips ahead of the line). (b) With the chin in normal horizontal relationship to the maxilla, the upper lip should be 3.5 mm and the lower lip 2.5 mm ahead of Sn-Pog′. (c) Effect in an individual with mandibular prognathism (lips on the line). In all three cases, the upper lip position has not changed; however, a change in Pog′ position results in a change in the lip position relative to the Sn-Pog′ line.
Labiomental fold
The lower lip–chin contour should have a gentle S-curve, with a lower lip–chin angle of at least 130 degrees (Fig 2-32). The angle is often acute in patients with Class II mandibular anteroposterior deficiency because of impingement of the maxillary incisor on the lower lip or macrogenia. The angle is flattened in individuals with microgenia or lower lip tension caused by Class III malocclusion. The surgeon considering genioplasty should assess not only the anteroposterior position of the Pog' but also the chin shape and the labiomental fold.

Fig 2-32Labiomental fold. The lower lip–chin angle should be at least 130 degrees.
Nasolabial angle
The nasolabial angle, which is measured between the inclination of the columella and the upper lip (Fig 2-33), should be in the range of 85 to 105 degrees ( Table 2-4). In females, a slightly larger angle is acceptable; whereas in males, a smaller angle is considered esthetically pleasing. Patients with mandibular anteroposterior deficiency have increased nasolabial angles, and this angle is usually acute in individuals with Class III occlusion. Surgical or orthodontic retraction of maxillary incisors should be avoided in individuals with large nasolabial angles. Where crowding necessitates tooth extraction, the nasolabial angle should influence the decision to extract first versus second premolars. Surgical repositioning of the maxilla also affects the nasolabial angle. In general, the maxilla should never be moved posteriorly, especially in combination with superior repositioning. This surgical movement leads to loss of lip support, increase in nasolabial angle, increase in nasal projection, and flattening of the nasal base. These changes result in poor esthetics and a premature aging effect. The maxilla should be moved posteriorly only in individuals with true maxillary protrusion, which occurs very rarely.
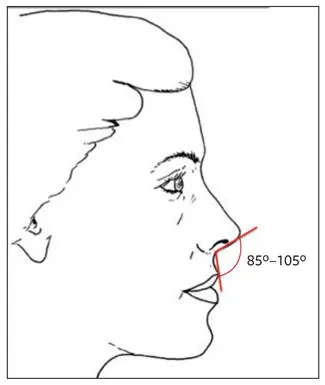
Fig 2-33The nasolabial angle, measured between the inclination of the columella of the nose and the upper lip, should be 85 to 105 degrees.
Table 2-4| Comparison of acute and obtuse nasolabial angles
| Acute angle | Obtuse angle | |
| Maxillary incisor position | Protruding | Upright or retroinclined |
| Nasal projection | Drooping nasal tip | Prominent or hanging columella |
| Occlusion | Class III | Class II |
| Bite | Deep bite | Open bite |
| Maxillary vertical dimension | Deficient | Excessive |
Chin
Although the chin forms a prominent esthetic feature of the face, it has no clearly defined function. Anatomically the chin is considered to be the soft tissue structure below the labiomental fold. Chin projection should be in good balance with the entire profile. The anteroposterior position of Pog', however, is not the only determining factor for good chin esthetics. When examining the chin, the clinician should consider the entire complex of structures forming the lower third of the face from Sn to Me'. It is difficult to isolate individual parts constituting this complex because the examiner should evaluate the size, shape, and position of each structure in relation to the other structures as well as the chin complex in relation to the rest of the face. At this stage, the middle third of the face should be masked and the relationship of the chin to the rest of the facial structures evaluated. Various soft tissue cephalometric analyses are available to assist in clinical evaluation of the anteroposterior chin position. However, the chin should be evaluated in all three dimensions. The width of the chin should be assessed in relation to the overall facial shape. A narrow chin often has a knobby appearance, and if surgical advancement of the chin is planned, widening of the chin should be contemplated. The labiomental fold, chin shape, relationship to the dental midline, symmetry, and cant of the lower border should be considered.
Chin-throat area
The presence of a double chin and adipose tissue should be noted. The lower lip–chin-throat angle (normally 110 degrees) provides chin definition (Fig 2-34). The distance from the neck-throat angle to Pog' (submandibular length) should be approximately 42 mm. These observations are pertinent when considering mandibular setback or advancement procedures, genioplasty (advancement or reduction), or submental liposuction ( Table 2-5).
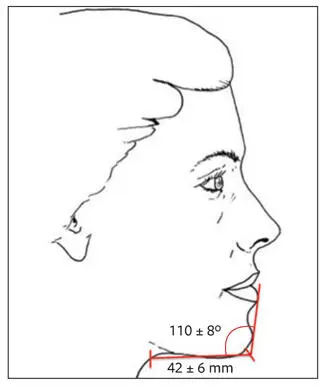
Fig 2-34Lip-chin-throat angle and submandibular length.
Table 2-5| Comparison of acute and obtuse lip-chin-throat angles
| Acute angle | Obtuse angle | |
| Mandibular anterposterior dimension | Excessive | Deficient |
| Submandibular fat | None | Present |
| Occlusion | Class III | Class II |
Radiographic Evaluations
Lateral Cephalometric Radiographic Evaluation
The information from lateral and (if indicated) posteroanterior cephalometric radiographs forms an important part of the database for orthognathic surgical treatment planning. Although clinical evaluation must be the primary diagnostic tool in determining surgical treatment of the orthognathic patient, cephalometric analysis is a helpful diagnostic guide. It enables the clinician to quantify, classify, and communicate dentofacial deformities; create a treatment plan via a visual treatment objective; help plan for tooth extractions; monitor progress during treatment; study specific changes during and after treatment to evaluate treatment results; and study facial growth.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.