Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The lateral cephalometric radiograph should be taken with the patient’s head in a natural posture, the teeth in centric occlusion, and the lips in repose. There are three exceptions to this requirement:
1 Where there is a clinically significant difference between the centric occlusion and centric relation, a second radiograph should be taken with the teeth in centric relation.
2 In patients with maxillary vertical deficiency, a second radiograph should be taken with the mandible rotated open until the lips just part. The maxillary incisor–upper lip relationship, upper lip length and shape, and the amount of maxillary downgraft can be more accurately evaluated on this radiograph.
3 In patients with severe Class III malocclusion and overclosed bites, it is difficult to assess the lips, tooth-lip relationship, and the relationship between the maxilla and mandible. A second radiograph should be taken with the mandible rotated until the lips just part.
The primary objective of treatment is not to make the patient’s cephalometric measurements normal, but rather to make the occlusal function normal and the facial appearance harmonious. For most patients, function and esthetics go hand in hand.
Cephalometric analysis involves measuring, comparing, and relating various linear and angular measurements of the hard and soft tissue structures of the face. The following analysis, a compilation of measurements useful in making a diagnosis and developing a treatment plan, is divided into lateral cephalometric analysis of soft tissue, hard tissue (skeletal analysis), and dental relationships.
Although soft tissue analysis is discussed as part of cephalometric analysis, it should be emphasized that the primary soft tissue examination of the facial esthetics guided by cephalometric analytic values should be done clinically. A patient’s cephalometric analysis and photographs should be part of the permanent records, but controlled, reliable records of the clinical examination are necessary for accurate diagnosis and correct treatment. The diagnosis should not be based only on the examination of photographs and cephalometric analysis.
Soft tissue analysis
Soft tissue landmarks
Lateral soft tissue landmarks, shown in Fig 2-35, include the following:
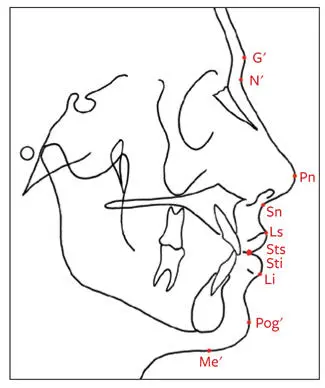
Fig 2-35Soft tissue cephalometric landmarks.
Soft tissue glabella (G′): The most anterior point of the forehead
Soft tissue nasion (N′): The deepest point of concavity in the midline between the forehead and the nose
Pronasale (Pn): The most anterior point of the nose
Subnasale (Sn): The point at which the columella of the nose merges with the upper lip in the midsagittal plane
Labrale superior (Ls): The mucocutaneous border of the upper lip vermilion
Stomion superius (Sts): The lowest point of the vermilion of the upper lip
Stomion inferius (Sti): The uppermost point of the lower lip vermilion
Labrale inferior (Li): The mucocutaneous border of the lower lip
Soft tissue pogonion (Pog′): The most anterior point of the chin in the midsagittal plane
Soft tissue menton (Me′): The lowest point on the contour of the soft tissue chin, found by dropping a perpendicular line from a horizontal line through the skeletal menton
Soft tissue planes
Soft tissue planes are shown in Fig 2-36 and include the following:

Fig 2-36Soft tissue planes. (1) Facial plane. (2) Upper facial plane. (3) Lower facial plane. (4) S-line. (5) E-line (esthetic plane).
Facial plane: Extends from N' to Pog′
Upper facial plane: Extends from G' to Sn
Lower facial plane: Extends from Sn to Pog'
S-line: Formed by connecting Pog' to a point midway between Pn and Sn
E-line: Extends from Pn to Pog'
Soft tissue vertical evaluation
Relationship of middle to lower facial third height
The distance from G' to Sn (middle facial third height) and from Sn to Me' (lower facial third height) is measured. The ratio should be approximately 1:1. In most orthognathic surgical patients, abnormalities are in the lower third of the face (Sn-Me'). In patients in whom the lower third of the face is increased in relation to the upper third, either vertical maxillary excess or an increase in the vertical anterior height of the mandible should be expected (Fig 2-37). A decrease in lower vertical height could be caused by either vertical maxillary deficiency, vertical deficiency of the anterior mandible, or an overclosed bite.
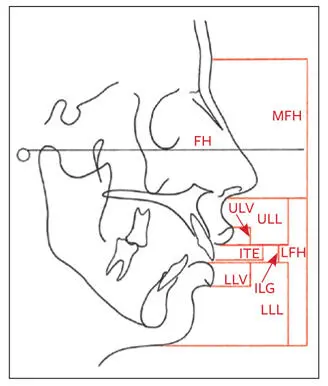
Fig 2-37Soft tissue vertical evaluation. Vertical measurements are made perpendicular to the FH plane. MFH, middle facial third height; ULV, upper lip vermilion height; ULL, upper lip length; ITE, incisor tooth exposure; LFH, lower facial third height; LLV, lower lip vermilion height; ILG, interlabial gap; LLL, lower lip/chin length.
Upper lip length
Upper lip length measured from Sn to Sts should be 22 ± 2 mm for males and 20 ± 2 mm for females (see Fig 2-37). Patients with relatively long upper lips tend to have less maxillary incisor exposure, whereas individuals with short upper lips tend to have an increased interlabial gap with increased maxillary incisor exposure ( Table 2-6). When vertical repositioning of the maxilla is contemplated, upper lip length should be considered to plan the correct amount of superior repositioning of the maxilla for each individual.
Table 2-6| Comparison of increased and decreased lip lengths
| Increased lip length | Decreased lip length | |
| Maxillary incisor exposure | Decreased | Increased |
| Differential diagnosis | Vertical maxillary deficiency | Vertical maxillary excess |
| Smile | Toothless | Gummy |
| Lip seal | Adquate | Increased interlabial gap |
Lower lip/chin length
The lower lip/chin length is measured from Sti to Me' and should be 44 ± 2 mm for males and 40 ± 2 mm for females (see Fig 2-37). An increase in the vertical dimension may indicate an increased anterior vertical height of the mandible. In contrast, a decrease may indicate a short anterior mandibular height. This dimension may also be short in individuals with both deep bites and everted lower lips.
Ratio of upper lip length to lower lip/chin length
The upper lip length (Sn-Sts) should be approximately half the length of the lower lip and chin (Sti-Me′; see Fig 2-37). A decrease in the vertical relation indicates either a long upper lip or a vertical deficiency of the anterior mandibular height. An increase in the ratio may be caused by either a short upper lip or a vertical excess of the anterior mandible.
Interlabial gap
When the lips are relaxed, they should be touching slightly, although an interlabial gap of 1 to 3 mm is still considered normal (see Fig 2-37). An increased interlabial gap (ie, larger than 4 mm) is usually an indication of lip incompetence due to vertical maxillary excess. Patients with a short upper lip, however, also tend to have an increased interlabial gap ( Table 2-7).
Table 2-7| Comparison of increased and decreased interlabial gaps
| Increased interlabial gap | Decreased interlabial gap | |
| Maxillary incisor exposure | Increased (assess with teeth in occlusion and lips relaxed) | None or little |
| Smile exposure | Gummy | Less than the full incisor crown exposed |
| Lip competence | Mouth breathing | Overclosed appearance |
| Vertical maxillary dimesnion | Excessive | Deficient/deep bite |
| Upper lip | Short | Long |
| Vermilion exposure | Excessive | Less |
Maxillary incisor exposure
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.