Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Chin prominence
Soft tissue chin prominence can be evaluated by measuring the distance to a line drawn through N' perpendicular to the FH. This line is also known as 0-degree meridian ; Pog' should be 0 ± 2 mm ahead of it (Fig 2-41). A more prominent chin would be more than 2 mm ahead of the 0-degree meridian, whereas a horizontally deficient chin would be more than 2 mm posterior to the line.
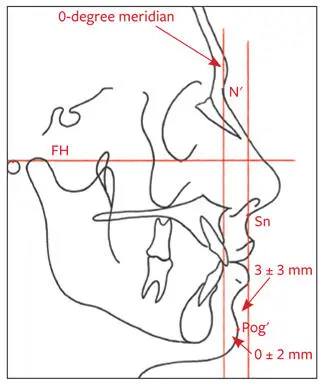
Fig 2-41Chin prominence. Anteroposterior evaluation of the chin to the 0-degree meridian and to a line perpendicular to the FH through Sn. Pog′ should be 0 ± 2 mm ahead of the 0-degree meridian and 3 ± 3 mm behind the SnV.
Another vertical line that is helpful in assessing the horizontal prominence of the chin is a line drawn perpendicular to FH through Sn. Pog' should be 3 ± 3 mm behind this line (see Fig 2-41). A horizontally excessive chin would be on or ahead of the vertical line, whereas a deficient chin would be more than 6 mm posterior to this line.
It is extremely important, however, to use the above measurements only as a guide when assessing chin position. Chin prominence must be evaluated in conjunction with other factors, such as chin shape, depth of the labiomental fold, microgenia, macrogenia, lower lip position, and mandibular anteroposterior excess or deficiency.
Lower lip–chin–throat angle
The lower lip–chin–throat angle is contained between a line drawn from Li to Pog' and a submental tangent line. An angulation of 110 ± 8 degrees is considered normal. For this assessment, the radiograph must be taken in natural head posture (Fig 2-42). This angle will be more acute in patients with mandibular anteroposterior excess and/or macrogenia. It will be more obtuse in cases of mandibular anteroposterior deficiency and/or microgenia.
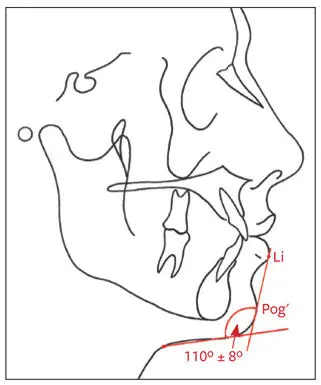
Fig 2-42Lower lip–chin–throat angle.
Chin-throat length
The chin-throat length is measured from the angle of the throat to Me′ (Fig 2-43). A distance of 42 ± 6 mm is considered normal. This measurement is only meaningful with the patient’s head in natural posture. The distance will be excessive in individuals with mandibular prognathism and short in those with a recessive mandible ( Table 2-9). This measurement is significant in differentiating between mandibular anteroposterior excess and maxillary deficiency. Mandibular setback would obviously reduce this length.
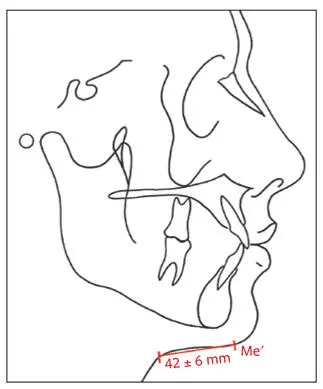
Fig 2-43Chin-throat length.
Table 2-9| Comparison of increased and decreased chin-throat lengths
| Increased chin-throat length | Decreased chin-throat length | |
| Mandibular anteroposterior dimension | Excessive | Deficient |
| Occlusion | Class III | Class II |
| Chin | Macrogenia | Microgenia |
Facial contour angle
The angle of facial convexity is formed by lines drawn from G′ to Sn and from Sn through Pog′. The line from G′ to Sn is also called the upper facial plane , whereas the lower facial plane is formed by the line from Sn to Pog′. The mean angulation is estimated to be –12 degrees. A clockwise angle is expressed as positive; a counterclockwise angle is negative. Males tend to have a straighter profile (–11 ± 4 degrees); a slightly more convex profile is considered esthetically pleasing for females (–13 ± 4 degrees; Fig 2-44a). It is important, however, to differentiate among the various facial deformities that may produce the same facial contour angle. The measurement of the angle does not reveal the localization of the deformity.
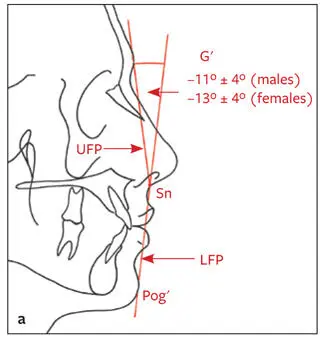
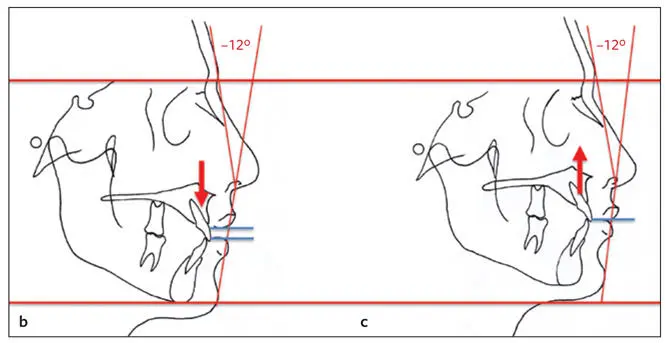
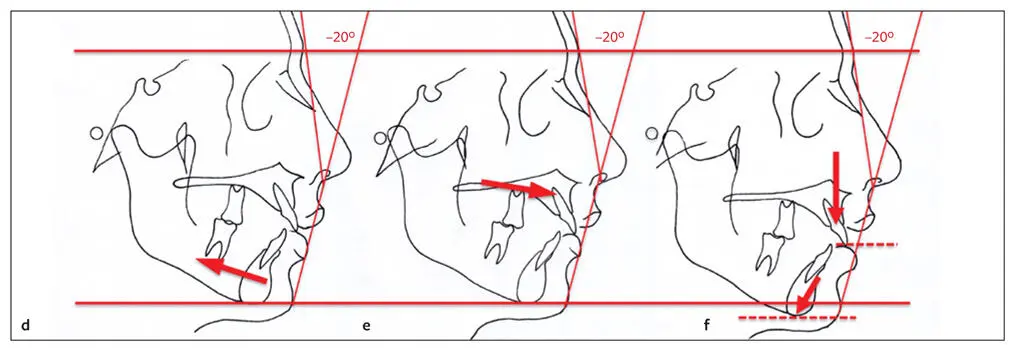
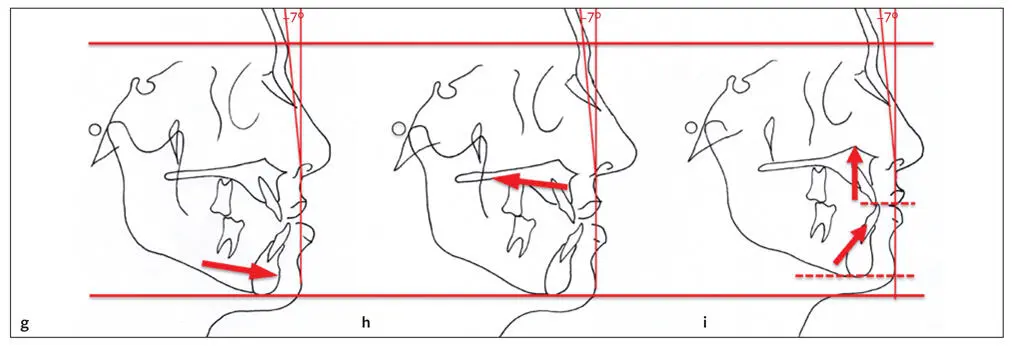
Fig 2-44 (a) Facial contour angle. (b and c) Both individuals have a facial contour angle of –12 degrees, but they have different vertical deformities. (b) Vertical maxillary excess. (c) Vertical maxillary deficiency. (d to f) The facial contour angle in all three individuals is –20 degrees, indicating a convex profile. The convexity, however, is caused by different deformities: (d) mandibular anteroposterior deficiency, (e) maxillary anteroposterior excess, and (f) vertical excess of the maxilla with clockwise mandibular rotation. (g to i) The facial contour angle in all three individuals is –7 degrees. This concavity is caused by different deformities: (g) mandibular anteroposterior excess, (h) maxillary anteroposterior deficiency, and (i) maxillary vertical deficiency with counterclockwise mandibular rotation.
In Figs 2-42b and 2-44c, both individuals have normal anteroposterior relations according to the facial contour angle (ie, –12 degrees). However, the vertical height of one is long (see Fig 2-44b), and the mandible has rotated clockwise; the other has a short vertical height (see Fig 2-44c) due to maxillary anteroposterior deficiency with the mandible rotated counterclockwise.
In Figs 2-44d to 2-44f, all three patients have a Class II malocclusion and an increased facial contour angle (ie, –20 degrees). Their identical facial contour angles, however, are produced by entirely different skeletal patterns. Figure 2-44d shows mandibular anteroposterior deficiency. Figure 2-44e shows maxillary anteroposterior excess, and Fig 2-44f shows vertical maxillary excess, with clockwise (backward) rotation of the mandible.
Figures 2-44g to 2-44i show Class III malocclusion and a more concave profile with decreased facial contour angle (ie, –7 degrees) produced by three entirely different skeletal patterns. Figure 2-44g shows mandibular anteroposterior excess. Figure 2-44h shows maxillary anteroposterior deficiency, and Fig 2-44i shows a maxillary vertical deficiency with counterclockwise (forward) rotation of the mandible.
E-line (Ricketts)
In relation to the E-line (Pn to Pog´), the upper lip should lie approximately 4 mm behind it whereas the lower lip should lie about 2 mm behind it (Fig 2-45). The profile contained by this line should form a reasonably symmetric Cupid’s bow. Dental support for the upper and lower lips will affect these values and distort the shape of the Cupid’s bow. In the assessment, the clinician should keep in mind the effect of the anteroposterior chin position (Pog′).
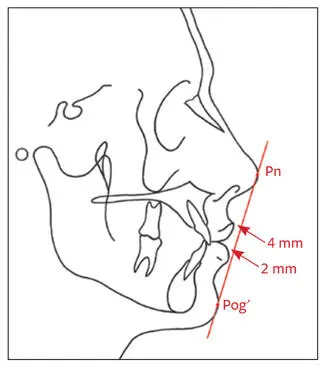
Fig 2-45E-line (Pn-Pog′).
S-line (Steiner)
The upper and lower lips should touch the S-line (drawn from Pog′ to the midpoint of the S-shaped curve between Sn and Pn; Fig 2-46). Lips behind this line may indicate lack of lip support or a prominent chin. Lips may fall ahead of this line because of dental protrusion or a deficient chin.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.