Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
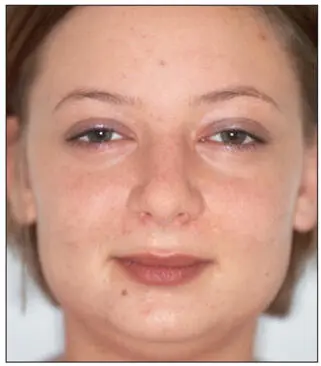
Fig 2-6In this individual, the bigonial width is greater than the bizygomatic width because of bilateral masseter muscle hypertrophy.
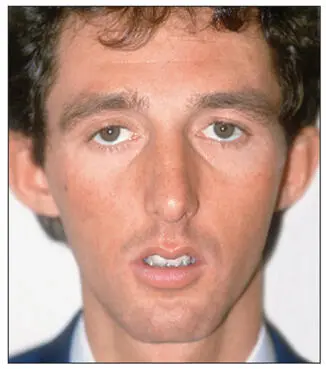
Fig 2-7Individual with a long, narrow face. The bizygomatic width is more than 30% greater than the bigonial width.
Transverse dimensions
The rule of fifths is a convenient method for evaluating transverse facial proportions. The face is divided into five equal parts—each the approximate width of the eye—from helix to helix of the outer ears (Fig 2-8).
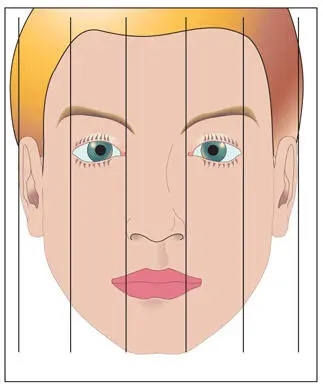
Fig 2-8Transverse facial proportions.
Table 2-1| Comparison of broad and narrow faces
| Broad face | Narrow face | |
| Facial height | Square, short | Long |
| Bigonial width | Masseter hypertrophy | Decreased intergonial distance |
| Nose | Broad nose | Narrow nose |
| Chin | Macrogenia | Microgenia |
The outer fifths are measured from the center helix of the ears to the outer canthus of the eyes. Prominent ears may have a profound effect on facial proportions and can be corrected by otoplasty. In patients with masseter hypertrophy, the face appears square, and the gonial angles fall well outside the canthus line. A more harmonious facial form can be established in these patients by means of bilateral reduction of the masseter muscles and contouring the mandibular angles (Fig 2-9). Intergonial width can be increased by subperiosteal angle implants (Fig 2-10).
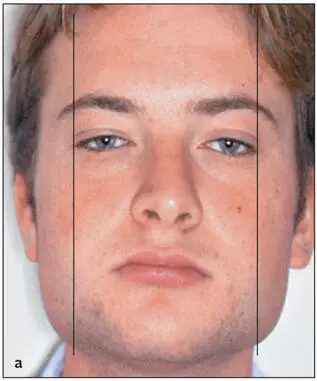
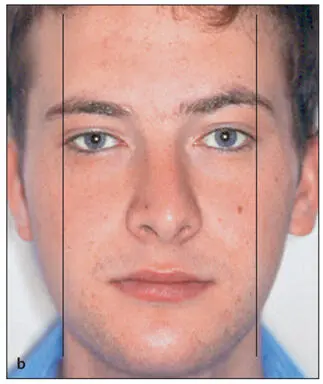
Fig 2-9 (a) The bigonial width is increased because of bilateral masseter muscle hypertrophy. The gonion falls lateral to a vertical line drawn through the outer canthus of the eye. (b) Transverse facial harmony has been restored by bilateral masseter muscle and mandibular angle reduction.

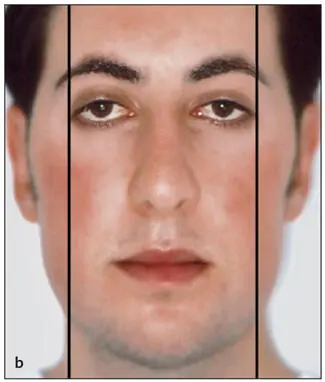
Fig 2-10 (a) This patient wanted to make his oval face more square. (b) The angles of the mandible were augmented by the placement of bilateral subperiosteal angle implants.
The medial three-fifths of the face are measured from the outer to the inner canthus of the eyes. The outer border should coincide with the gonial angles of the mandible. In patients with masseter muscle hypertrophy, the gonial angles will fall well lateral to this line (see Fig 2-9a). In patients with long faces, there will be a tendency for the gonial angles to be medial to these lines. It should be noted that the width of the mouth should approximate the distance between the inner margins of the irises of the eyes (Fig 2-11).
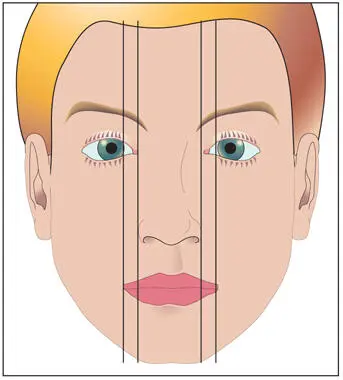
Fig 2-11Vertical lines drawn through the medial canthi should coincide with the ala of the nose, whereas vertical lines drawn through the medial margins of the irises of the eyes should coincide with the corners of the mouth.
The middle fifth is delineated by the inner canthus of the eyes. In patients with hypertelorism, this fifth will be out of proportion with the other four-fifths. The ala of the nose should coincide with these lines (see Fig 2-11). For patients in whom maxillary advancement and/or superior repositioning is considered and the ala falls outside of the lines, control of alar width is indicated during surgery (see chapter 5).
Facial symmetry
To assess facial symmetry, an imaginary line is drawn through the soft tissue glabella (G'), pronasale (Pn), center of the philtrum of the upper lip and lower lip, and soft tissue pogonion (Pog'; Fig 2-12). For more accurate assessment, these points should be marked on the patient’s face one at a time while other parts of the face are blocked out.
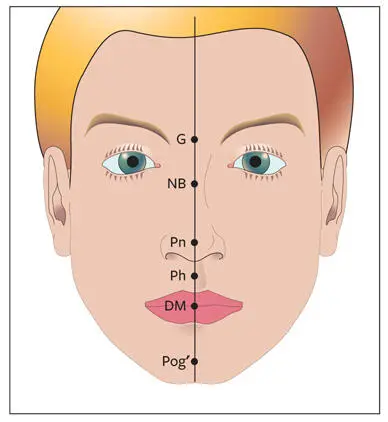
Fig 2-12Facial symmetry. Important midline structures are the midpoint between the eyebrows (G), nasal bridge (NB), nasal tip (Pn), midpoint of the philtrum of the upper lip (Ph), dental midlines (DM), and midpoint of the chin (Pog').
The maxillary and mandibular dental midlines should be assessed in relation to the facial midline, as well as in relation to each other. These observations will play an important role in the decision-making process regarding surgical or orthodontic correction of dental midlines. It is also important to evaluate the mandibular dental midline in relation to the midline of the chin. This information will assist in treatment planning for correction of mandibular asymmetry by means of mandibular surgery, genioplasty, or both. The presence of a transverse cant in the occlusal plane should be noted and correlated with the asymmetry. Surgical correction of an occlusal plane cant will often play a significant role in the total correction of facial asymmetry and should not be corrected orthodontically (see chapter 4).
No face is perfectly symmetric, but the absence of any obvious asymmetry is necessary for good facial esthetics. Posteroanterior cephalometric radiography or CBCT imaging for 3D virtual treatment planning are indicated in the presence of a clinically significant asymmetry. This will allow the clinician to distinguish between bone, soft tissue, or a combination of the two as etiologic factors.
Vertical relationship
In the vertical dimension, the face can be divided into three equal parts (Fig 2-13): (1) upper third (hairline [trichion] to the glabellar area), (2) middle third (glabellar area to subnasale [Sn]), and (3) lower third (Sn to soft tissue menton [Me']).
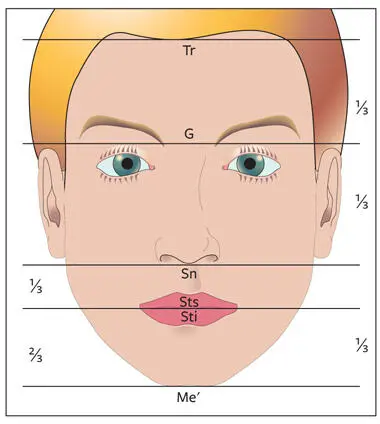
Fig 2-13The face is divided into thirds by drawing horizontal lines through the trichion (Tr), G, subnasale (Sn), and soft tissue menton (Me'). The lower third can be divided into an upper third (from Sn to stomion superius [Sts]) and a lower two-thirds (from stomion inferius [Sti] to Me').
Upper third of the face
Fortunately, deformities that exist in the upper third of the face can usually be masked by an appropriate hairstyle. However, it is important to record deformities in this area because they may indicate craniofacial deformities.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.