Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Consultation with Other Disciplines
Consultation with practitioners in other disciplines may be needed in the treatment of patients with a dentofacial deformity.
Periodontics
In general, most periodontal diseases should be treated prior to orthodontic banding. The teeth and periodontium should be sound before treatment. The importance of oral hygiene during the orthodontic treatment phase should be stressed, and the possibility of periodontal treatment after debanding should be mentioned to the patient.
Prosthodontics
Any work on fixed partial dentures is preferably performed after a period of orthodontic retention. However, it is often advantageous for the patient to consult with a prosthodontist before beginning treatment. The prosthodontist can contribute valuable insight into certain aspects of the surgical/orthodontic treatment and prosthodontic rehabilitation. For example, in a patient with congenitally missing lateral incisors, should the interdental spaces be closed, or should spaces be maintained and the missing teeth be replaced by implants or fixed partial dentures? For edentulous patients or those with a limited number of teeth that would not require orthodontic treatment, the preoperative prosthodontic consultation is mandatory.
Implant dentistry
It is often possible to place the necessary implants at the time of orthognathic surgery. It is important, however, to keep any postoperative orthodontic tooth movement in mind. Dental implants can often be placed more accurately after band removal and a short period of retention. However, it will be more expensive for the patient to undergo two separate surgeries. For patients requiring bone grafts before implants can be placed, the surgeon should consider placing the bone grafts during orthognathic surgery.
General dentistry
Problems such as dental caries, fractures, periodontitis, and poor-fitting crowns should be addressed before treatment begins. The condition of certain teeth may influence the decision of which teeth are extracted for orthodontic reasons. The initial referral to the orthodontist or surgeon is often made by the general practitioner, and it is important to keep him or her informed of the treatment plan and the progress of the patient’s treatment. The general practitioner should be part of the treatment team.
Importance of communication
Accurate treatment planning and meticulous orthodontic and surgical practice are essential to the achievement of treatment objectives. Just as important, however, is communication between the clinician and the patient, as well as between clinicians. It is crucial to have adequate communication between the orthodontist, patient, and surgeon about the patient’s main complaint and concerns, dentofacial diagnosis, treatment possibilities, and treatment objectives (Fig 1-7). The confident sharing of information with the patient will build trust between patient and clinician. Remember, people want to know how much you care before they care how much you know.
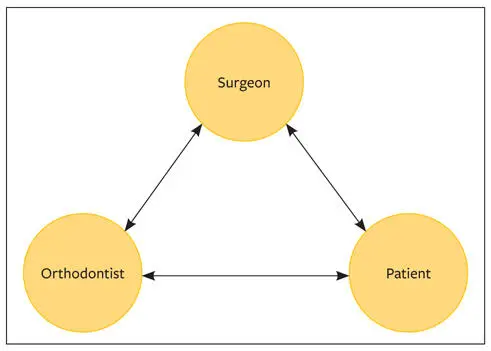
Fig 1-7Kindness, communication, and free flow of information between the surgeon, orthodontist, and patient facilitate efficient and successful treatment and ensure patient confidence.
The communication between the surgeon and the orthodontist is equally important. Lack of communication here not only hampers the development of an efficient and sound treatment plan but also generally leads to poor treatment results. Patients are extremely concerned about poor or lacking communication between the orthodontist and the surgeon, and it can lead to confusion. Clinicians should refrain from sending messages to each other via the patient.
Treatment plan
The development of a treatment plan has three advantages:
1 It represents an agreement between the orthodontist and the surgeon on how the patient will be treated.
2 The treatment plan and objectives can confidently be presented to the patient without contradictions.
3 Although the treatment plan may be changed when indicated, it serves as a solid guideline.
The treatment plan may need to be revised or changed after the preoperative orthodontic treatment is under way. The reason for a change in treatment plan and the solution should be discussed by the orthognathic team so that there will be no surprises during the immediate preoperative surgical consultation. Superb orthodontic alignment of teeth and excellent surgical technique do not substitute for good clinical judgment, optimal decision making, proper communication, and empathy with patients.
Recommended Reading
Arnett GW, McLaughlin RP. Facial and Dental Planning for Orthodontists and Oral Surgeons. St Louis: Mosby, 2004.
Bell WH. Modern Practice in Orthognathic and Reconstructive Surgery, vol 1. Philadelphia: Saunders, 1992.
Enlow DH. Facial Growth, ed 3. Philadelphia: Saunders, 1990.
Epker BN, Stella JP, Fish LC. Dentofacial Deformities: Integrated Orthodontic and Surgical Correction, vol 1. St Louis: Mosby, 1994.
Gasparini G, Boniello MD, Moro A, Di Nardo F, Pelo S. Orthognathic surgery: A new preoperative informed consent model. J Craniofac Surg 2009;20:90–92.
Naini FB. Facial Aesthetics: Concepts & Clinical Diagnosis. Wiley-Blackwell, 2007.
Proffit WR, White RP. Surgical Orthodontic Treatment. St Louis: Mosby, 1990.
Sarver DM, Proffit WR, White RP. Contemporary Treatment of Dentofacial Deformities. St Louis: Mosby: 2002.
Spalding PM. Craniofacial growth and development. In: Miloro M, Ghali GE, Larsen P, Waite P (eds). Peterson’s Principles of Oral and Maxillofacial Surgery, ed 3. Shelton, CT: People’s Medical Publishing House-USA, 2012:1189–1238.
Wolford LM, Stevao ELL, Alexander CM, Goncalves JR, Rodrigues DB. Orthodontics for orthognathic surgery. In: Miloro M, Ghali GE, Larsen P, Waite P (eds). Peterson’s Principles of Oral and Maxillofacial Surgery, ed 3. Shelton, CT: People’s Medical Publishing House-USA, 2012:1263–1294.
There must be clear and effective communication between the orthodontist and the maxillofacial surgeon from the outset of treatment to achieve the best results from surgical therapy. Through this close relationship, a full exchange of information and data can be made. Each practitioner involved in the patient’s care should be familiar with the standard records required, and the data on the patient should be shared regardless of who actually performs the investigations. Treatment should commence only after both the orthodontist and the surgeon have consulted with the patient, a treatment plan has been jointly prepared, and both clinicians have a copy of the patient’s records. Orthognathic surgeons should have a thorough understanding of orthodontic treatment principles to enable them to communicate sensibly, to plan realistically, and to know what can be expected from the orthodontic treatment. Conversely, orthodontists should understand the surgical possibilities, limitations, and requirements to make the partnership ultimately advantageous to the patient.
A systematic examination is necessary to adequately evaluate and plan treatment for patients with dentofacial deformities. In routine cases, this evaluation includes the following:
General patient evaluation
Sociopsychologic evaluation
Esthetic facial evaluation
Radiographic evaluationLateral cephalometricPosteroanterior cephalometricFull-mouth periapicalPanoramic
Occlusion and study cast evaluation
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.