Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Selecting a treatment
Patients seeking orthodontic treatment have a wide range of functional and esthetic needs and can be divided into three groups (Fig 1-1):
Group 1: Those with a normal skeletal relationship and malocclusions that can be treated using routine orthodontic techniques.
Group 2: Those with mild to moderate skeletal discrepancies. The malocclusions of many of the patients in this group can be corrected by dental compensation and growth management. Both options—pursuing only orthodontic treatment and pursuing combined treatment—will have advantages and disadvantages that must be discussed between the clinicians, the patient, and the patient’s parents (if necessary). There are several factors that will determine the treatment decision.
Group 3: Those with moderate to severe skeletal discrepancy and noticeable facial imbalance. The negative effects of compromised orthodontic treatment for patients in the third group would be unacceptable, making combined surgery and orthodontics the treatment of choice. In cases when the surgical option is not acceptable to the patient, it would be wise for the surgeon not to accept the patient for treatment. Orthodontic treatment alone for patients in this group will certainly worsen the esthetics, have doubtful stability, and possibly have negative long-term periodontic implications (Figs 1-2 and 1-3). On the other hand, only pursuing surgery without orthodontics would also lead to compromise.
An important challenge for the clinician is to differentiate between patients on the borderline between group 2 and group 3. An orthodontic camouflage treatment for patients in group 3 would be a mistake, just as surgical treatment of certain patients in group 2 would be inappropriate. The decision regarding the best treatment for borderline patients is influenced by various factors:
The patient’s main complaint and preferences. Some patients are interested only in improving occlusion, whereas esthetic change is a high priority for others. The patient’s priority is an important factor in treatment planning: The patient needs to be able to weigh the two treatment options against each other and must therefore be well informed.
1 Long orthodontic treatment. This often involves headgear, functional appliances, and a different extraction pattern with a compromised treatment outcome. The possibility of worsening esthetics, instability, and long-term periodontal problems should be discussed with the patient (and parents when applicable).
2 Shorter orthodontic treatment combined with surgery. The surgical implications, possible complications, and improved treatment outcome must be discussed with the patient (and parents when applicable).
The orthodontist’s preferences and skills. If the orthodontist has encountered poor surgical results with previous patients, there will be a natural hesitation to continue to recommend surgery. The orthodontist’s confidence in the success of surgery is an important factor.
Available surgical skills. Orthognathic surgical expertise may not be available in the area, and the patient may be unable to travel.
Lack of insurance coverage. The financial implications of orthodontic treatment with the added burden of surgery and hospitalization can be substantial, and this is a significant factor for patients to consider.
Treating patients in group 3 with orthodontics alone (group 2 treatment) may create additional problems (eg, occlusal relapse, worsening of the profile, obstructive sleep apnea (OSA), periodontal and temporomandibular joint decline) rather than solving the existing problem. Surgical treatment of patients in group 2 is appropriate when camouflage treatment would produce an unacceptable esthetic result or when orthodontics alone cannot achieve the desired facial change. Camouflage treatment also can be considered an alternative treatment method that should render acceptable functional, stable, and esthetic results.
Treatment Objectives in Orthognathic Surgery
Four treatment objectives are fundamental in orthognathic surgery: (1) function, (2) esthetics, (3) airway patency, and (4) stability of results. These objectives form the basic goals in treating patients with dentofacial deformities and often go hand in hand.
Function
Functional and esthetic deformities often exist concurrently, so treatment should be designed to correct both. The orofacial functional objectives should not only incorporate the bite and chewing functions but also include normal breathing, speech, swallowing, and temporomandibular joint function. When correcting a functional problem, the clinician should make full use of the opportunity to improve facial esthetics at the same time. It is particularly challenging to treat patients whose function is poor but esthetics are already good. Careful planning is essential to avoid additional esthetic deformity while providing optimal functional relationships.
Esthetics
The patient’s main concern is often their facial appearance, and it is paramount to establish what the patient perceives as esthetically wrong. As Leo Tolstoy said in Childhood , “I am convinced that nothing has so marked influence on the direction of a man’s mind as his appearance, and not his appearance itself so much as his conviction that it is attractive or unattractive.”
Esthetic imbalance is often the result of a significant dentoskeletal deformity. Esthetic results can be improved by surgery alone in some patients, although the functional problem will not necessarily be treated. For example, if a patient with mandibular anteroposterior deficiency is treated with surgical advancement of the chin, this may result in a Class II malocclusion. In contrast, for a patient with vertical maxillary excess, it may be possible to achieve a Class I occlusion by orthodontic treatment alone; however, an ideal esthetic result is not possible.
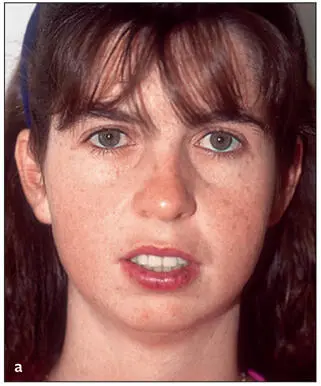
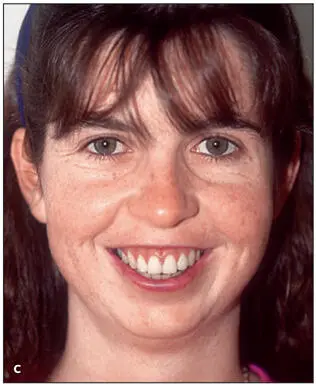
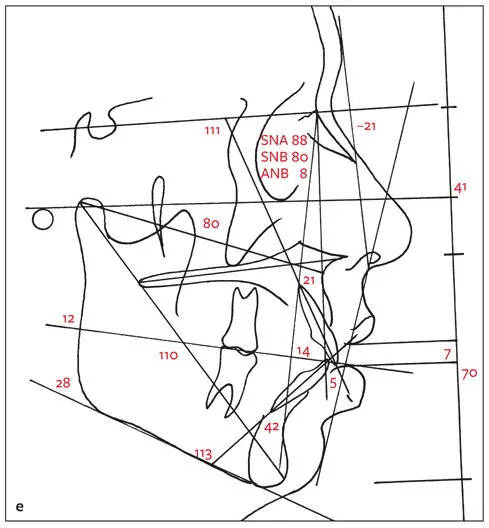
Because the orthodontic placement of the teeth dictates surgical movement (and ultimately facial changes), the orthodontist must carefully assess patients with musculoskeletal deformities before orthodontic treatment is begun. Accurate preoperative orthodontic and surgical planning that considers the indicated surgical movement is necessary to ensure not only good functional results but also an optimal esthetic outcome. As seen in the patient in Fig 1-4, the dentition has been compromised for skeletal vertical maxillary excess and mandibular anteroposterior deficiency. Function and questionable stability have been achieved; however, the esthetic result is poor. An acceptable result is achieved after surgical compromise.





Интервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.