Johan P. Reyneke - Essentials of Orthognathic Surgery
Здесь есть возможность читать онлайн «Johan P. Reyneke - Essentials of Orthognathic Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essentials of Orthognathic Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essentials of Orthognathic Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essentials of Orthognathic Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essentials of Orthognathic Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essentials of Orthognathic Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
When people recognize malpositioned teeth or obvious jaw deformities, they usually seek treatment from an orthodontist, who can improve tooth alignment, function, and facial esthetics. More severe deformities that require a combination of orthodontics and surgery for correction are called dentofacial deformities . These deformities can affect physical orofacial function in several ways. Mastication can be impaired, and—especially in severe cases—this impairment can affect digestion and general nutritional health. Lip incompetence due to excessive vertical growth of the maxilla results in mouth breathing, which eliminates the physiologic effect of the nose on breathing. Speech is often affected by dentofacial deformities despite the body’s adaptive capabilities. Malpositioned teeth may have a profound effect on proper oral hygiene maintenance, making teeth more susceptible to dental caries and periodontal disease. The patency of the airway and normal breathing is certainly affected by the position of the jaws, and dentofacial deformities are currently considered an important etiologic factor in the development of obstructive sleep apnea. Several types of dentofacial deformities also affect temporomandibular function. The physical effects of a dentofacial deformity are important, but the psychosocial impact of a dentofacial deformity on an individual is often paramount. This type of deformity can profoundly affect the quality of life and may entail lifelong adjustment.
Treatment Options for Dentofacial Deformities
The combination of surgery and orthodontic treatment makes it possible to treat dentofacial deformities that are not possible to correct with orthodontics alone (eg, vertical maxillary excess and severe anterior open bite malocclusion). Orthognathic surgery has created new and exciting opportunities in the treatment of patients with dentofacial deformities and provided the orthodontist with options other than compromised treatment for patients with skeletal disharmony. Experience in orthognathic surgery, an increased understanding of its biologic basis, and a refinement of its art form now enable us to routinely deliver a stable, esthetic, and functional result to patients. When severe skeletal discrepancies result in malocclusion, three kinds of treatment are available: growth modification, orthodontic camouflage, and orthognathic surgery.
Growth modification
This treatment approach should only be considered for mild skeletal deformities. In growing children, dentofacial orthopedics can alter the expression of growth to some extent. However, the extent of growth alteration varies, and this topic remains controversial. The following facial growth patterns may be influenced by growth modification in adolescents:
Maxillary anteroposterior excess: Excessive horizontal growth of the maxilla may be impeded by headgear or camouflaged by extraction of the maxillary first premolars and orthodontic retraction of the incisors.
Maxillary anteroposterior deficiency: Moderate improvement can be established by orthodontic protraction.
Vertical maxillary excess: High-pull headgear with temporary anchorage devices can impede the vertical growth of the maxilla and diminish the severity of the deformity.
Mandibular anteroposterior deficiency: Headgear combined with functional appliances may improve mandibular projection.
Skeletal deformities such as mandibular anteroposterior excess, vertical maxillary deficiency, and microgenia cannot be easily influenced by growth modification. In addition, there are some patients who may undergo growth modification for a long period of time with headgear or elastics and end up still requiring a surgical approach. This can be very disappointing and frustrating for the patient as well as their family and health care providers.
Preparing for surgery in these cases would often also require “reverse” orthodontics, decompensating the attempts to compenstate the dentition before orthognathic surgery, prolonging treatment even further.
Orthodontic camouflage
Certain patients with mild skeletal discrepancies would benefit from orthodontic camouflage rather than surgery. Dental compensation for a skeletal deformity, or orthodontic camouflage, may, however, be associated with impaired esthetics, questionable posttreatment stability, and prolonged treatment time (see Figs 1-2 and 1-3). Corrective treatment may require rebanding and a second orthodontic treatment followed by orthognathic surgery.

Fig 1-1Patients who may seek treatment for their malocclusions from an orthodontist can in general be divided into three categories according to the severity of their skeletal deformities. When planning treatment, it can be challenging but is essential to differentiate between groups 2 and 3.
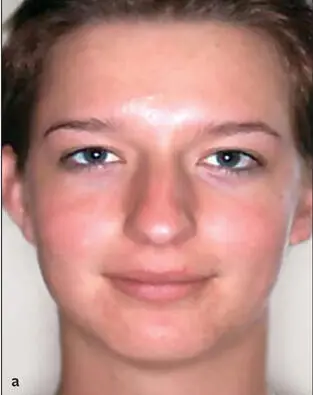





Fig 1-2 (a to f) A 19-year-old patient with a skeletal Class II relationship who would be considered to fall into group 3. Her maxillary first premolars were removed and the maxillary incisors retracted in an attempt to correct her occlusion. Unfortunately, the treatment compromised her esthetics and occlusion, resulting in a severe convex profile that accentuated her prominent nose and a Class II deep bite malocclusion.
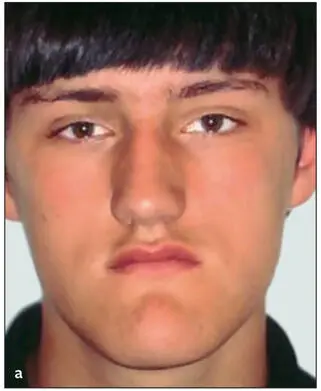
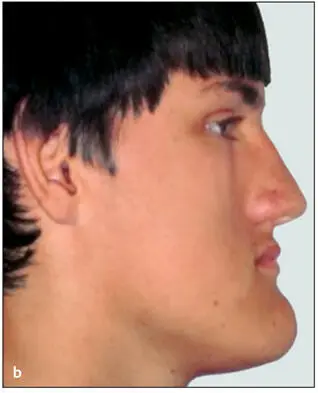

Fig 1-3 (a to c) A 16-year-old patient with a skeletal Class III relationship. His four premolars were removed at a younger age, and an attempt was made to establish an occlusion with orthodontic treatment. This is an example of a patient that would fall into the group 3 category; however, he was treated with orthodontics only.
Orthognathic surgery
Combined orthodontic and surgical correction is considered the best treatment modality for dentoskeletal imbalances once growth has ceased. Although orthognathic surgery is associated with certain risks and challenges, it has become a more refined and less traumatic procedure for patients and therefore is now a reasonable treatment option. Improving skeletal relationships will result in remarkable facial changes, and this is an important goal to consider.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essentials of Orthognathic Surgery»
Представляем Вашему вниманию похожие книги на «Essentials of Orthognathic Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Essentials of Orthognathic Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.