Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Courtesy of Robert M. Fulton, DVM, Richmond, VA.
Reverberation or A‐Lines: Strong Reflector (Air)
Reverberation occurs when sound encounters two highly reflective layers. The sound is bounced back and forth between the two layers before traveling back to the receiver. The probe will detect a prolonged traveling time and assume a longer traveling distance and display additional reverberated images in a deeper tissue layer. The reverberations can get caught in an endless loop and extend all the way to the bottom of the screen as parallel equidistant lines, referred to as A‐lines (also see Chapters 22and 23). This artifact most commonly extends beyond air‐filled structures within the thorax, (e.g., lung) and within the abdomen (e.g., gastrointestinal tract), with varying width (Penninck 2002) ( Figure 3.5; see also Figures 3.1and 3.2).
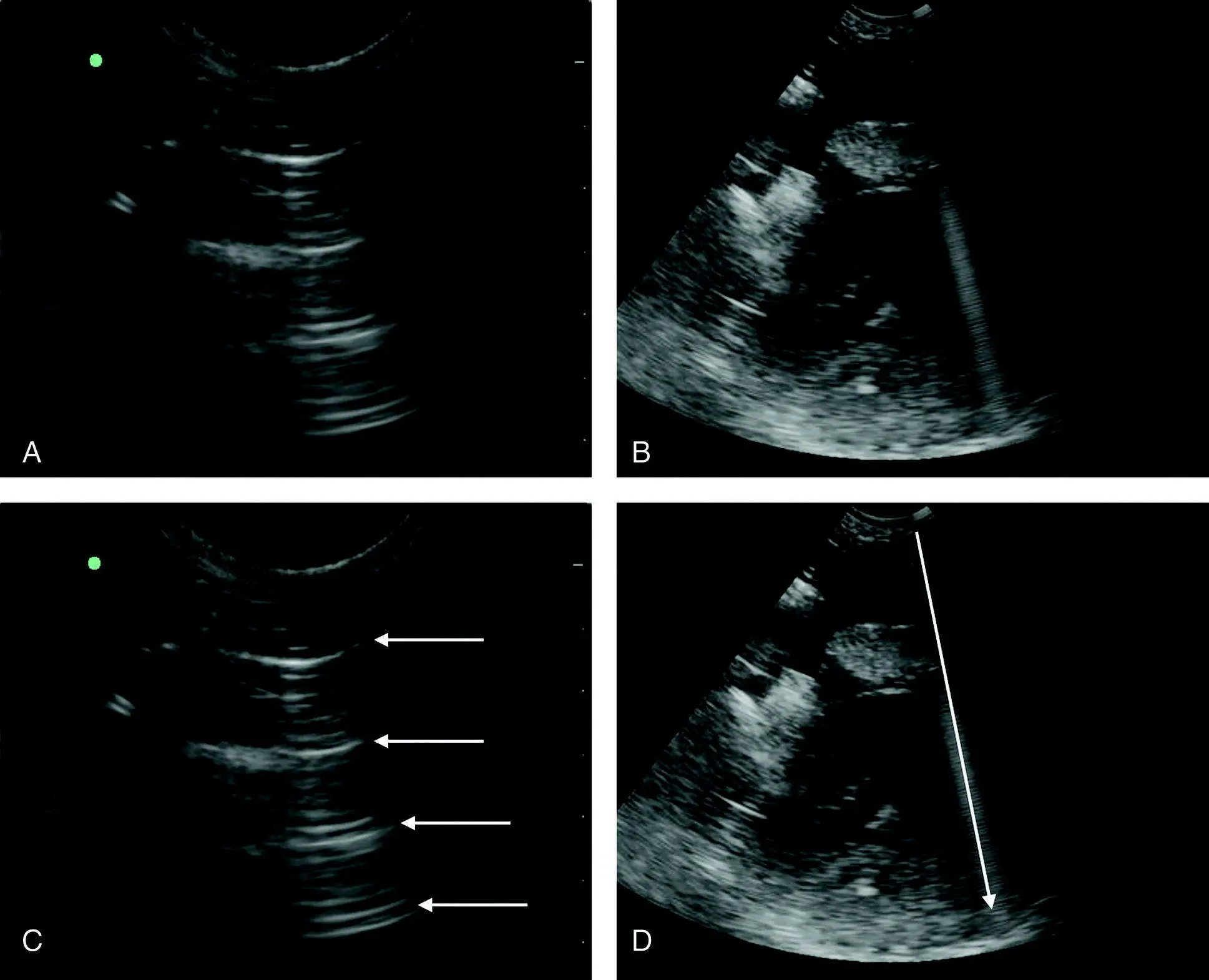
Figure 3.5. Reverberation artifact. (A) Reverberation artifact, also known as A‐lines (think of it as "A" for air). A‐lines are seen as regularly spaced parallel lines illustrated by the arrows (←) outlined in (C). The most proximal arrow in the near‐field denotes the lung's surface, evident within the intercostal space between two ribs on either side (ribs [bone] creating the "clean shadowing" through the far‐field). (B) The very tight and distinct band of reverberation artifact, referred to as a comet‐tail or ring‐down artifact, caused by sound waves reflecting off a metal needle used during abdominocentesis in the near‐field. (D) The same image but with an arrow overlay to show the tight band of A‐lines as the comet‐tail or ring‐down artifact. Any strong reflector of ultrasound waves produces this artifact that typically involves bone, stone, or metal, such as implants, needles, and foreign bodies.
Source: Courtesy of Robert M. Fulton, DVM, Richmond, VA.
Comet‐Tail or Ring‐Down Artifact: Strong Reflector (Usually Metal or Bone But Can Be Air)
A comet‐tail artifact, also called a ring‐down artifact, is similar to reverberation. It is produced by the front and back of very strong reflectors with high acoustic impedance, such as metallic foreign bodies or implants, needles, and stylets during ultrasound‐guided procedures (see also Chapters 43and 44), or strong reflectors with very low acoustic impedance relative to their adjacent soft tissues, such as gas in the lung, gas bubbles, or gas in the bowel. The reverberations are spaced very narrowly and blend into a small band. The greater the difference between the acoustic impedance of the reflecting structure and the surrounding tissues, the greater the number of reverberation echoes (Reef 1998) (see Figure 3.5).
B‐Lines: Strong Reflector (Air Immediately Next to Fluid)
Ultrasound lung rockets (ULRs), more recently termed B‐lines (Volpicelli et al. 2012), are vertical, narrow‐based lines arising from the near‐field's pulmonary–pleural line, extending to the far edge of the ultrasound screen, always obliterating A‐lines, and moving “to and fro” in concert with inspiration and expiration. Although B‐lines are similar to comet‐tail artifacts, they are specifically created by the strong difference in impedance of air adjacent to a small amount of water and are the ultrasound near‐equivalent of radiographic Kerley B lines (representing interlobar edema). Their clinical relevance is very important and explained later (see Chapters 22and 23) (Lichtenstein and Meziere 2008; Lichtenstein et al. 2009; Lisciandro 2011; Volpicelli et al. 2012) ( Figure 3.6).
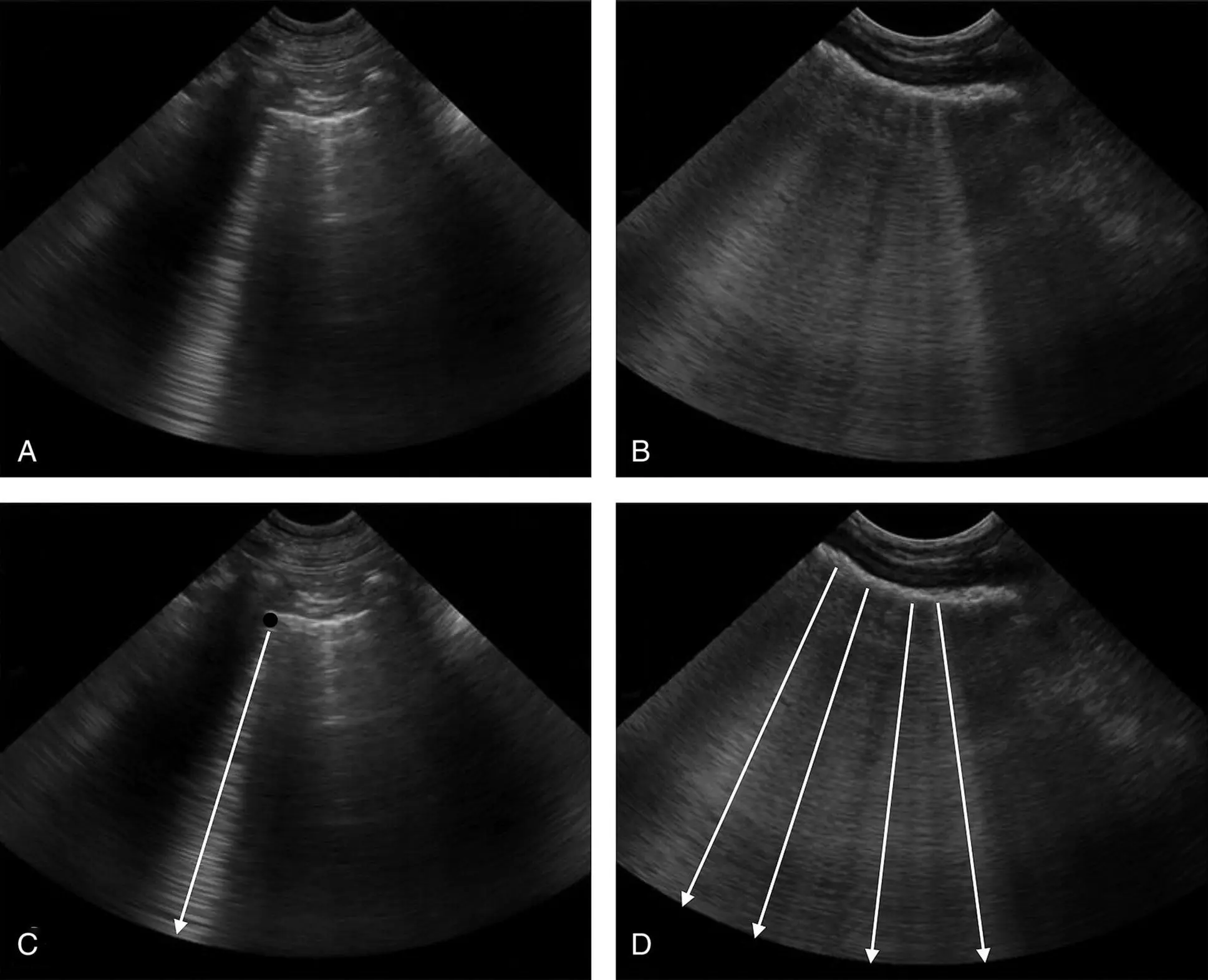
Figure 3.6. Pseudo B‐lines. The B‐line artifact begins at the lung's pleural surface and continues without loss of intensity through the far‐field of the image as a hyperechoic (bright white) streak that obliterates A‐lines. In real time, B‐lines must oscillate with the to‐and‐fro motion of inspiration and expiration. Examples and descriptions are found in Chapters 22and 23. Here, however, are pseudo B‐lines. In (A), what appears to be a single B‐line is in fact tightly stacked A‐lines off the far side of a very small lung nodule. In (B) are multiple pseudo B‐lines off the gastric wall. In (C) the nodule is indicated with a solid black circle overlay, and the arrows are over the pseudo B‐line. In (D), the pseudo B‐lines are indicated by the arrows (←).
Source: Courtesy of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Artifacts of Multiple Echoes
Side‐Lobe Artifact: Multiple Echoes
We like to think of the ultrasound beam as extending from the probe in a very thin fan or rectangle, and this is exactly what the processor thinks it sees. In reality, there are smaller beams that travel laterally to the main beam. When one of these smaller side beams is of sufficient strength and bounces off a highly reflective surface, such as the wall of the urinary bladder, it will be interpreted as coming from the main beam and the processor will place the resulting image within the main beam image, often mimicking sediment. The resulting image is usually weaker in intensity than the main image. Often, the artifact can be altered by changing probes or lowering the focal point, or lowering the gain setting – all ultrasonographic manipulations that will not remove true pathology (i.e., bladder sediment, bladder stones, etc.) (Penninck 2002) ( Figure 3.7).
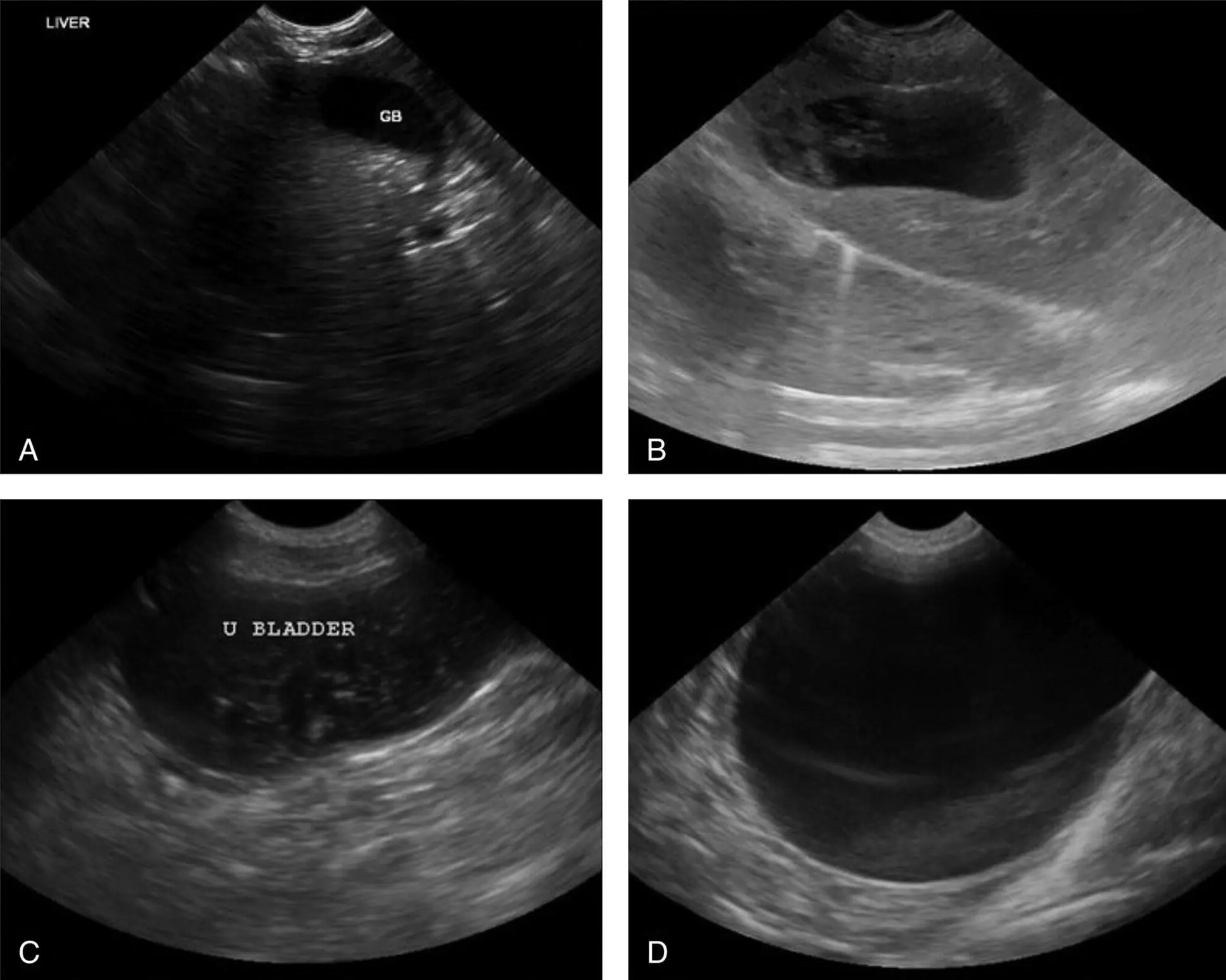
Figure 3.7. Sediment versus side‐lobe and slice‐thickness artifact. (A) Sediment will be affected by gravity and lead to a flat surface, as seen with the sludge within this gallbladder's lumen. True sediment can be stirred up by repositioning the patient or through ballottement with the ultrasound probe, whereas artifacts mimicking sediment cannot. (B) Slice‐thickness and side‐lobe artifacts mimic sediment in the gallbladder shown here; however, the artifact will not be altered by moving the patient's position or by ballottement. (C) True sediment in a urinary bladder with ballottement gives a snow globe appearance. (D) In contrast, the slice‐thickness and side‐lobe artifacts mimicking sediment shown here will fail to ballot (will not "snow globe") or change position to the gravity‐dependent side of the urinary bladder when the patient is moved. Other helpful tricks that discriminate true sediment from artifact include lowering the gain and/or moving the focus cursor. Generally speaking, artifacts can be eliminated by these maneuvers, but true sediment cannot.
Source: Courtesy of Robert M. Fulton, DVM, Richmond, VA.
Slice‐Thickness Artifact: Multiple Echoes
Slice‐thickness artifact is somewhat like the side‐lobe artifact. In the gallbladder and urinary bladder in particular, this artifact mimics sludge or sediment. It occurs when part of the beam's thickness lies just outside a fluid‐filled structure. These artifacts typically appear within the lumen of these structures and are somewhat hyperechoic (bright) and curved. They can be differentiated from real sediment by several methods or clues. First, gravity‐dependent sediments have a flat surface whereas the artifact will be rounded. Second, by changing the position of the patient, the relative position of true sediment will change as gravity pulls it to the new lower point. Third, the sonographer can use the ultrasound probe to ballot the bladder and stir the sediment up a bit; the artifact will not yield a “snow globe” effect (sediment will) (Penninck 2002) (see Figure 3.7).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.