James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Armamentarium
Laboratory knife with no. 25 blade
Horseshoe wax wafers
Plaster bowl
Technique
The patient is guided into a CRCP closure, and the position of the mandibular midline in relation to the maxillary teeth is visually noted. The points on the maxillary teeth that would be opposite the mandibular midline if the patient moves the mandible 5.0 mm in both a right and left lateral excursion are measured and marked with a pencil ( Fig 4-23). With a hand on the patient’s chin, the dentist asks the patient to open slightly. The dentist then guides the mandible approximately 5.0 mm to the right and closes it until the teeth lightly touch. The dentist explains that this procedure will be repeated with some wax between the teeth and that the patient should bite down carefully until told to stop.
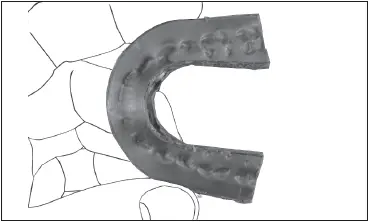
Fig 4-25The lateral interocclusal record has been trimmed before use.
A slightly warmed wax wafer (Surgident Coprwax Bite Wafer, Heraeus Kulzer) is placed against the maxillary teeth approximately 4.0 mm to the right of center. Using one hand to support the wax, the dentist guides the mandible to the right. The closure practiced previously is repeated until the teeth make indentations in the wax approximately 1.0 mm deep ( Fig 4-24). The wax wafer is cooled with compressed air, removed from the mouth, and placed in a plaster bowl of cold tap water. The steps are repeated with a second wax wafer on the left side. After the wax wafer has cooled, a sharp laboratory knife is used to carefully cut off any of the wax that extends distal to the marginal ridge of the most posterior mandibular tooth on both sides of the wafer ( Fig 4-25). This ensures that the wax wafer will completely seat on the mandibular cast when the articulator condylar inclination is set. The bite registrations are then rinsed with a hospital-grade disinfectant and placed in an unsealed sterilization bag until ready to be used.
References
1. Lucia VO. Centric relation: Theory and practice. J Prosthet Dent 1960;10:849–856.
2. Lucia VO. A technique for recording centric relation. J Prosthet Dent 1964;14:492–505.
3. Hobo S, Iwata T. Reproducibility of mandibular centricity in three dimensions. J Prosthet Dent 1985;53:649–654.
4. Williamson EH, Steinke RM, Morse PK, Swift TR. Centric relation: A comparison of muscle-determined position and operator guidance. Am J Orthod 1980;77:133–145.
5. McHorris WH. Centric relation defined. J Gnathol 1986;5:5–21.
6. Dawson PE. Temporomandibular joint pain-dysfunction problems can be solved. J Prosthet Dent 1973;29:100–112.
7. Dawson PE. Evaluation, Diagnosis, and Treatment of Occlusal Problems. St Louis: Mosby, 1974:58.
8. Perry HT. Muscular changes associated with temporomandibular joint dysfunction. J Am Dent Assoc 1957;54:644–653.
9. Weinberg LA. Physiologic objective of reconstruction techniques. J Prosthet Dent 1960;10:711–724.
5 Articulation of Casts
To properly evaluate a patient’s occlusion, it is mandatory that diagnostic casts be placed in an articulator in approximately the same relationship to the temporomandibular joints (TMJs) as that which exists in the patient. 1A facebow registration is used to mount the maxillary cast on the articulator so that it is properly located both anteroposteriorly and mediolaterally. 2,3To be used enough to make a real contribution to the improvement of quality dentistry, a facebow and articulator that possess reasonable accuracy, are simple to assemble and use, and can be set up relatively quickly should be selected.
Information collected in an informal manufacturer’s survey of the 67 North American dental schools indicated that 31 schools were using a Whip Mix articulator, 29 were using a Hanau (Whip Mix), 4 were using a Stratos (Ivoclar Vivadent), and 3 were using a Panadent. Models used varied among the schools, and some schools used one brand of articulator for one discipline and another brand for a different discipline. Each of the following sections on a facebow-articulator combination is meant to stand alone (ie, everything the reader needs to know about the use of a system is contained in that respective section). The one exception lies in the description of a mechanical anterior guide. Although similar devices are available for all three articulators, use of the mechanical anterior guide is described only for the Hanau articulator.
Whip Mix Facebow and Articulator
The technique for the QuickMount facebow with Quick Lock Toggle (Whip Mix) ( Fig 5-1), an ear facebow that possesses the qualities previously described, is presented. Following that is the technique for the use of the Whip Mix 2200 series articulator, a semi-adjustable instrument. Casts mounted on one of these articulators can be transferred accurately to another instrument of the same type that has been set to the same parameters. 4There are many advantages to this feature, including the ability to send casts to the laboratory without sending the instrument. 5
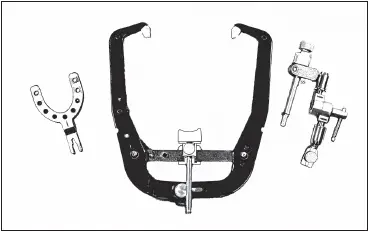
Fig 5-1The components of a QuickMount facebow are (left to right) a bite fork, the facebow with the nasion relator, and the Quick Lock Toggle assembly.
Facebow armamentarium
QuickMount facebow (with bite fork, nasion relator, and Quick Lock Toggle assembly)
Whip Mix articulator
Plaster bowl
Spatula
Laboratory knife with no. 25 blade
Trimmed maxillary cast
Horseshoe wax wafers
Mounting stone (Whip Mix)
Facebow record technique
Two horseshoe wax wafers (Surgident Coprwax Bite Wafer, Heraeus Kulzer) are heated in warm tap water until they become soft and flexible. A wafer is adapted to each side of the bite fork so that it is uniformly covered (Fig 5-2). The wax-covered bite fork is placed against the maxillary teeth. The attachment portion of the fork is centered on the patient’s midline. The bite fork is supported, and the patient is instructed to close lightly into the wax to obtain shallow impressions of only the cusp tips ( Fig 5-3). The wax is cooled, and the bite fork is removed from the mouth. Excess wax is trimmed away. Any areas where soft tissue was registered on the wax must be completely removed.
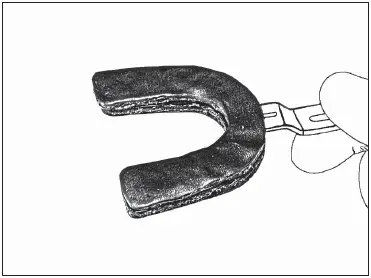
Fig 5-2A wax wafer has been adapted to each side of the bite fork.
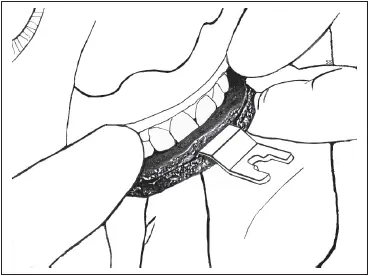
Fig 5-3The bite fork is placed against the maxillary teeth and supported by the dentist as the patient closes lightly for a shallow impression of the cusp tips.
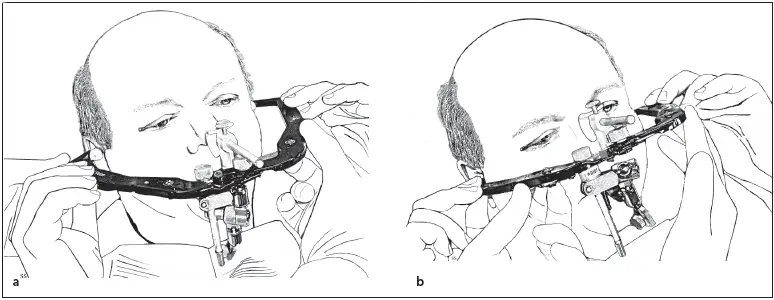
Fig 5-4The patient guides the earpieces (a) as the dentist places them into the external auditory meati (b) .
The maxillary cast is set in the bite fork registration to confirm that the cast seats firmly in the index with no rocking or instability. If the cast does not seat, first the occlusal surfaces of the cast are checked to make sure there are no nodules of stone. If there are none, then either the registration or the cast is distorted and should be remade.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.