James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The medial pair of clamp thumbscrews on the top or backside of the upper frame of the articulator are loosened slightly. Both condylar guides are set at 0 degrees ( Fig 5-28). The lateral translation clamp screws on the forward aspect of each condylar guide are loosened, and the immediate lateral translation controls are set at their most open position ( Fig 5-29). The incisal guide pin is raised so that it will not touch the plastic incisal stop in any position.
The upper frame, with cast attached, is inverted, and the right lateral interocclusal record is seated on the teeth of the maxillary cast. The teeth should seat completely in the wax indentations. The upper frame is held in the left hand, and the right condylar element is placed in the right condylar guide. The teeth of the mandibular cast are gently positioned in the indentations of the wax record. They must be seated completely. The articulator is supported in this position with one hand on the right side. The left condylar element will have moved downward, forward, and inward. It is not touching the condylar guide at any point ( Fig 5-30).
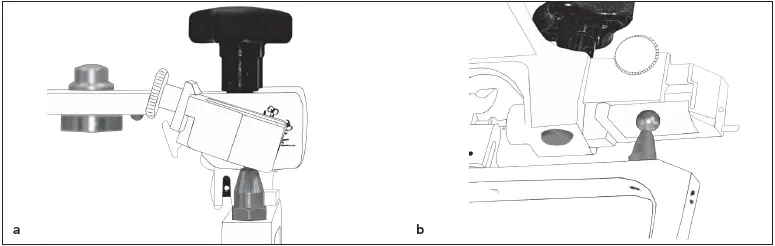
Fig 5-30With the right lateral interocclusal record in place, the left condyle does not contact the superior wall (a) or the medial wall (b) of the guide.
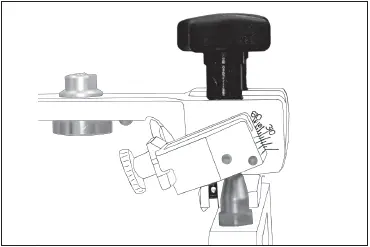
Fig 5-31The condylar inclination is increased until the condyle contacts the superior wall of the guide.
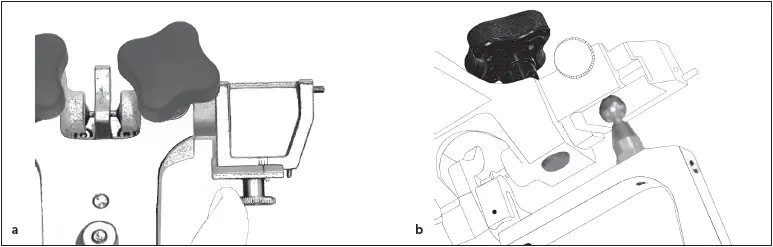
Fig 5-32The medial wall of the guide is moved (a) until it contacts the condyle (b) .
The inclination of the left guide is set by releasing its clamp screw. The guide is rotated inferiorly until the superior wall again touches the condylar element ( Fig 5-31). The holding screw is tightened. Mandibular lateral translation is accommodated by releasing the lateral translation clamp screw and sliding the lateral translation guide laterally until it touches the medial surface of the condylar element ( Fig 5-32). The clamp screw is retightened. The right condylar guidance is set by using the record for the left lateral excursion and repeating these steps.
Once the lateral interocclusal records have been made for the diagnostic mounting and the articulator has been set, the data is recorded on the patient’s information card. On the patient’s casts, the correct articulator settings for each side are marked. For example, a condylar inclination of 40 degrees and a lateral translation of 0.3 mm would be recorded as 40/0.3. When teeth are prepared at a future date and working casts are mounted on the articulator, it will not be necessary to make new lateral interocclusal records. The recorded information from the diagnostic mounting can be used to set the instrument.
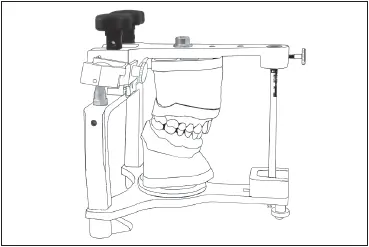
Fig 5-33The guidance provided by anterior teeth can be recorded in acrylic resin in the dovetail incisal block.
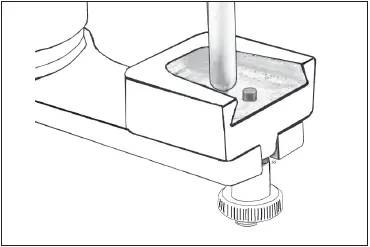
Fig 5-34The incisal guide pin is 2 to 3 mm posterior to the tip of the retaining screw.

Fig 5-35Tray resin is placed in the dovetail incisal block.
Anterior guidance
The influence of the TMJ on the occlusal scheme has been noted. The use of lateral interocclusal records in the setting of the condylar guides enables transfer of some of the influence from the TMJ to the semi-adjustable articulator. The influence of the incisors and canines (ie, anterior guidance) on the occlusion during excursive movements must also be taken into account. 6,7
The guidance given to mandibular movements by the anterior teeth can be recorded using either acrylic resin or a lightcured material such as Triad (Dentsply) and made part of the setting of the articulator ( Fig 5-33). Anterior guidance can, in effect, be transferred from the teeth to the incisal guide block of the articulator. If crowns restoring the lingual contours of the anterior teeth are to be placed, it is extremely important that the anterior guidance be registered on the articulator. If this is not done, the lingual contours or length of the restorations produced may not provide anterior guidance.
The mounted casts are examined on the articulator to assess the anterior guidance. If there are nonworking interferences on the casts, they are removed to enable the articulator to move freely while maintaining contact between the anterior teeth. The anterior guidance is examined to determine its adequacy. If it is not adequate because of wear, fracture, or missing teeth, it is restored to an optimum form with inlay wax or denture teeth on the cast.
The acrylic incisal block is replaced on the articulator with the dovetail incisal block (Whip Mix). The block is positioned so that the incisal guide, with the round end down, is 2 to 3 mm posterior to the tip of the retaining screw ( Fig 5-34). The round end of the incisal guide pin and the functioning surfaces of the anterior teeth are lubricated with petrolatum. The interior surface of the dovetail block is also coated. Onehalf scoop of tray acrylic resin is mixed in a paper cup. While it still flows freely, a small amount is placed in the interior of the block ( Fig 5-35). The material is allowed to acquire some body before proceeding.
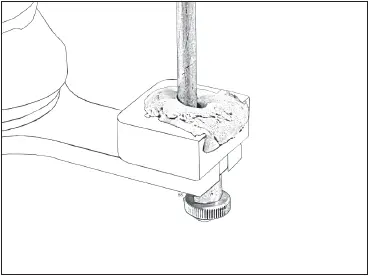
Fig 5-36The guide pin is closed into the soft acrylic resin.
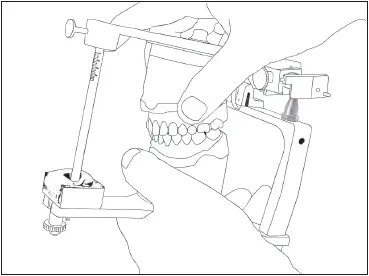
Fig 5-37The articulator is moved through all excursions.
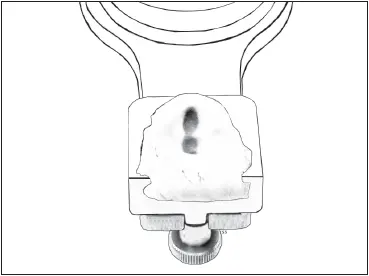
Fig 5-38An anterior guidance record has been formed in the dovetail incisal block.
The articulator is closed into full occlusion so that the guide pin penetrates into the soft tray resin ( Fig 5-36). The articulator is moved repeatedly through all the mandibular movements, making sure that the anterior teeth remain in contact at all times ( Fig 5-37). The tip of the incisal guide pin molds the acrylic resin to conform to the various movements. Movement of the articulator through all the excursions continues until the tray resin has polymerized.
Excess resin is trimmed off after it has polymerized. The tip of the guide pin has acted as a stylus in forming a registration of the anterior guidance ( Fig 5-38). It will now be possible to duplicate the influence of the anterior teeth on the movements of the casts, even if the anterior teeth are prepared and the incisal edges shortened.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.