James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
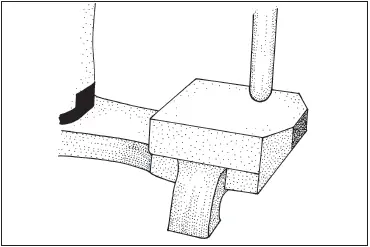
Fig 5-51The incisal guide pin should not contact the guide block.
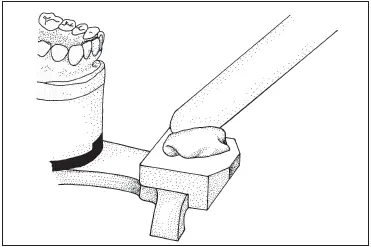
Fig 5-52Acrylic resin is placed on the incisal guide.
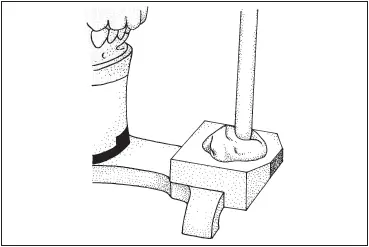
Fig 5-53The guide pin is allowed to close into the soft resin.
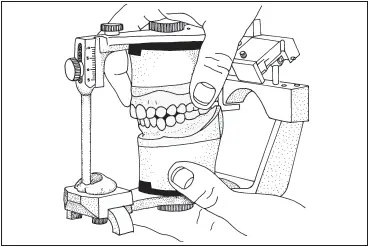
Fig 5-54The articulator is moved through all excursions.
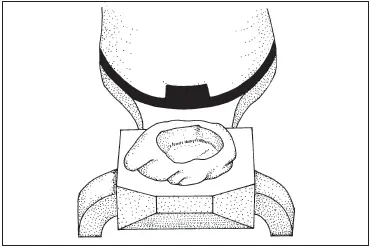
Fig 5-55An anterior guidance record exists on the guide block.

Fig 5-56The components of a Spring-Bow are (left to right) the facebow with orbital pointer and the bite fork assembly.
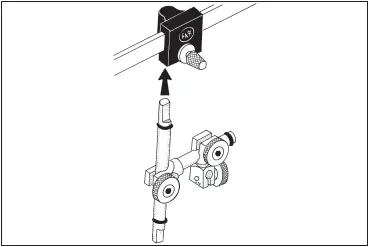
Fig 5-57The vertical rod of the bite fork assembly is inserted into the bow socket. The flat side is in front, with the empty bite fork clamp to the right.
Hanau Facebow and Articulator
The Hanau Spring-Bow (Whip Mix) is an ear facebow that utilizes a one-piece spring-steel bow ( Fig 5-56). It is simple in design and can be used either as a direct-mount or an indirect-mount device with the removable bite fork assembly and mounting platform. 8The technique for its use is described with the Hanau Series 184 Wide-Vue articulator (Whip Mix), an arcon semi-adjustable instrument.
Facebow armamentarium
Spring-Bow (with bite fork assembly and mounting guide)
Hanau Wide-Vue articulator
Plaster bowl
Spatula
Laboratory knife with no. 25 blade
Trimmed maxillary cast
Pink baseplate wax
Mounting stone
Facebow record technique
A sheet of baseplate wax is softened in hot water, and the bite fork is completely covered with it. The wax-covered bite fork is positioned against the maxillary teeth, and the patient is instructed to close until the mandibular teeth contact the wax on the underside of the fork. The shaft of the bite fork will be to the left of the patient’s midline.
The wax is cooled in the mouth with an air syringe. The fork is removed from the mouth and placed in a bowl of cold tap water to finish cooling. Excess wax and any areas imprinted by soft tissue are trimmed off. The maxillary cast is seated in the wax record to be sure that it is stable. If there is any rocking of the cast, the occlusal surfaces of the cast should be checked for nodules of stone. If there are none, either the cast or the record is distorted and must be remade.
If the bite fork assembly is separate from the facebow, the transfer (vertical) rod of the assembly is inserted into the bow socket on the underside of the black centerpiece on the front of the facebow. The flat surface on the rod must be in front when it is placed in the socket. The assembly should be on the right, with the knobs facing the front ( Fig 5-57). The thumbscrew is tightened on the front of the centerpiece.
While the patient grips the bite fork between the maxillary and mandibular teeth, the loosened bite fork clamp is positioned 4 cm (1.5 inches) over the bite fork shaft. The facebow should be pointed upward during this action ( Fig 5-58). The bow is opened by pulling outward on the arms and is swung down into position, with an earpiece placed gently into each external auditory meatus. The patient is instructed to adjust the earpieces to the most comfortable seated position ( Fig 5-59).
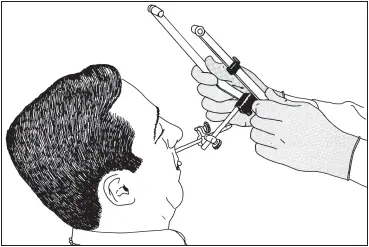
Fig 5-58The bite fork clamp is slid onto the shaft.
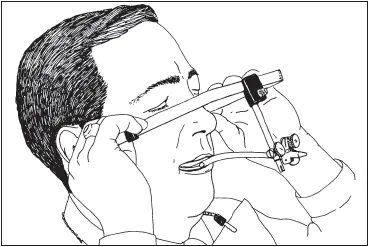
Fig 5-59The patient should adjust the facebow for comfort. The earpieces should be checked to make sure they are still seated.
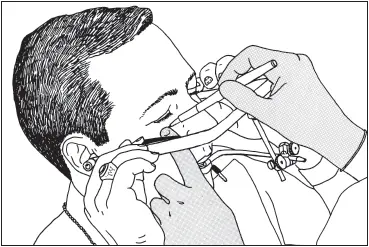
Fig 5-60The infraorbital notch (orbitale) is located and marked.
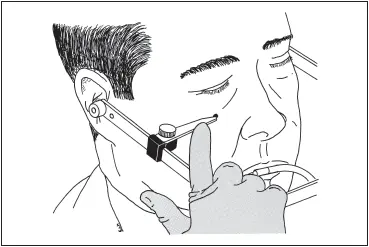
Fig 5-61The pointer is rotated toward the reference mark.
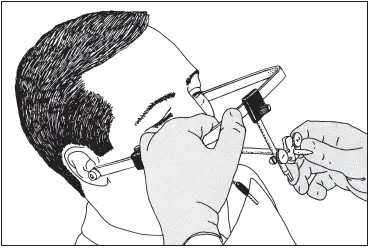
Fig 5-62The bow is secured with one hand while the other tightens the thumbscrews on the bite fork assembly.
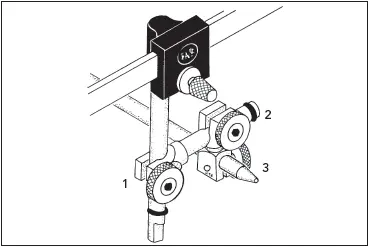
Fig 5-63The thumbscrews are tightened in the order indicated (1–3).
The orbitale (infraorbital notch) is marked on the patient’s face with a felt-tip marker to provide an anterior reference point ( Fig 5-60). The thumbscrew that holds the orbital pointer is loosened and gently swung in toward the reference mark ( Fig 5-61). The front of the facebow is elevated along the transfer (vertical) rod of the bite fork assembly until the pointer is at the plane of the anterior reference point. The bow is grasped to resist torquing ( Fig 5-62), and the three thumbscrews are tightened in order from left to right ( Fig 5-63):
1 Transfer (vertical) rod/transverse (horizontal) rod
2 Transverse rod clamp (upper)
3 Bite fork clamp (lower)
They must be tight; an Allen wrench can be used to tighten them if necessary.
The reference pointer is rotated back over the right temple of the bow, and the thumbscrew is tightened enough to hold it there. While the patient opens, the ends of the bow are grasped, and the earpieces are removed from the auditory meati. It should be held firmly because the bow is made of spring steel and could snap back. The bow is slid away from the patient. The facebow, earpieces, and bite fork are disinfected with a hospital-grade disinfectant before continuing.
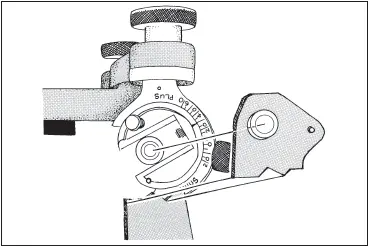
Fig 5-64Before the facebow is attached, the condylar inclination is set at 30 degrees.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.