James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
5. Sokolow SM. Interchangeable quick-mounted study models. J Clin Orthod 1986;20:779–781.
6. Weinberg LA. Physiologic objective of reconstruction techniques. J Prosthet Dent 1960;10:711–724.
7. Schuyler CH. The function and importance of incisal guidance in oral rehabilitation. J Prosthet Dent 1963;13:1011–1030.
8. Strohaver RA, Ryan JR. New face-bow simplifies use and dental laboratory cooperation. J Prosthet Dent 1988;60:638–641.
6 Treatment Planning for Single-Tooth Restorations
Using cast metal, ceramic, and metal-ceramic restorations, large areas of missing coronal tooth structure can be replaced while the remainder is preserved and protected. Function can be restored, and where required, a pleasing esthetic effect can be achieved. The successful use of these restorations is based on thoughtful treatment planning, which is manifested by choosing a restorative material and design that are suited to the needs of the patient. In a time when production and efficiency are heavily stressed, it should be restated that the needs of the patient take precedence over the convenience of the dentist.
In what circumstances should cemented restorations made from cast metal or ceramic be used instead of amalgam or composite resin restorations? The selection of the material and design of the restoration is based on several factors.
The first factor is destruction of tooth structure . If the amount of destruction previously suffered by the tooth to be restored is such that the remaining tooth structure must gain strength and protection from the restoration, cast metal or ceramic is indicated over amalgam or composite resin.
Esthetics is another important factor. If the tooth to be restored with a cemented restoration is in a highly visible area, or if the patient is highly discriminating, the esthetic effect of the restoration must be considered. Sometimes a partial coverage restoration will serve this function. Where full coverage is required in such an area, the use of ceramic in some form is indicated. Metal-ceramic crowns can be used for single-unit anterior or posterior crowns, as well as for fixed partial denture retainers. All-ceramic crowns are most commonly used on incisors, although they can be used on posterior teeth when an adequate amount of tooth structure has been removed and the patient is willing to accept the possibility of more frequent replacement.
Plaque control also plays a role. The use of a cemented restoration demands the institution and maintenance of a good plaque-control program to increase the chances for success of the restoration. Many teeth are seemingly prime candidates for cast metal or ceramic restorations, based solely on the amount of tooth destruction that has previously occurred. However, when these teeth are evaluated from the standpoint of the oral environment, they may, in fact, be poor candidates for cemented restorations. If extensive plaque, decalcification, and caries are present in a mouth, the use of crowns of any kind should be carefully weighed. The design of a restoration should take into account those factors that will enable the patient to maintain adequate hygiene to make the restoration successful. The patient must be motivated to follow a regimen of brushing, flossing, and dietary regulation to control or eliminate the disease process responsible for destruction of tooth structure. It may be desirable to use pin-retained amalgam provisional restorations to save the teeth until the conditions responsible for the tooth destruction can be controlled. This will give the patient the time necessary to learn and demonstrate good oral self-care. It will also permit the dentist and staff to reinforce the skills required of the patient and to evaluate the patient’s willingness and ability to cooperate. If these measures prove successful, cast metal, ceramic, or metal-ceramic restorations can be fabricated. Because these restorations are used to repair the damage caused by caries and do nothing to cure the condition responsible for the caries, they should not be used if the oral environment has not been brought under control.
A fourth factor is financial considerations . Finances influence all treatment plans because someone must pay for the treatment. That may be a government agency, a branch of the military, an insurance company, and/or the patient. If the patient is to pay, the dentist should provide good advice and then allow the patient to make the choice. A conscientious dentist must walk a fine ethical line. On the one hand, a dentist should not preempt the choice by selecting a less-than- optimum restoration just because he or she thinks that the patient cannot afford the optimum treatment. On the other hand, a dentist should be sensitive enough to the individual patient’s situation to offer a sound alternative to the optimum treatment plan and not apply pressure.
A final factor is retention . Full coverage crowns are unquestionably the most retentive 1,2( Fig 6-1). However, maximum retention is not nearly as important for single-tooth restorations as it is for fixed partial denture retainers. It does become a special concern for short teeth and removable partial denture abutments.
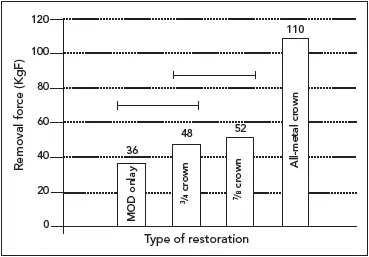
Fig 6-1A comparison of resistance to removal forces for four types of crowns ( P = .05) .1,2MOD, mesio-occlusodistal.
Twelve restoration types are presented in the following pages to provide a frame of reference for making a decision whether to use a “plastic” restoration or a cemented restoration. The plastic restoration is inserted as a soft (ie, plastic) mass into the cavity preparation, where it will harden and be retained by mechanical undercuts or adhesion. The cemented restoration, made of cast metal, metal-ceramic, or all-ceramic material, is fabricated outside of the operatory and is luted or bonded to the patient’s tooth at a subsequent appointment. One type can be better suited for a particular application than the other, or in some cases either may be suitable.
Intracoronal Restorations
When sufficient coronal tooth structure exists to retain and protect a restoration under the anticipated stresses of mastication, an intracoronal restoration can be employed. In this circumstance, the crown of the tooth and the restoration itself are dependent on the strength of the remaining tooth structure to provide structural integrity.
Glass ionomer
Small lesions where extensions can be kept minimal and where preparation retention will be minimal can be restored with glass ionomer. It is useful for restoring Class V lesions caused by erosion or abrasion ( Fig 6-2). It also can be employed for incipient lesions on the proximal surfaces of posterior teeth by use of a so-called tunnel preparation, which leaves the marginal ridge intact ( Fig 6-3).
Glass ionomer has found a niche in the restoration of root caries in geriatric and periodontal patients ( Fig 6-4). An occlusal approach may be precluded by the presence of an otherwise acceptable crown, or a conventional restoration at such an apical level might require the destruction of an unacceptable amount of tooth structure. In addition, handpiece access may be too restricted to create the needed retention for a small amalgam restoration.
Glass ionomer also can be placed rapidly enough to serve as an interim treatment restoration to assist in the control of rampant caries ( Fig 6-5). This is further enhanced by the release of fluoride by the material.
Composite resin
This material can be used for minor to moderate lesions in esthetically critical areas ( Fig 6-6). While it can be used in the restoration of incisal angles assisted by acid etching, a tooth that has received a Class IV resin restoration ultimately will require a crown.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.