James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
If a protrusive interocclusal wax record is used to establish the condylar inclination, both condylar mechanisms are rotated simultaneously in the same manner described above for setting each condylar inclination separately. In this situation, the angle of mandibular lateral translation (L) is esti- mated by use of the Hanau formula : L = H/8 + 12, where H is the condylar protrusive inclination. Because a change in condylar inclination from 20 to 50 degrees would produce less than a 4-degree change in the Bennett angle by this calculation, placing the Bennett angle ring at an arbitrary 15-degree angle would produce minimal error.
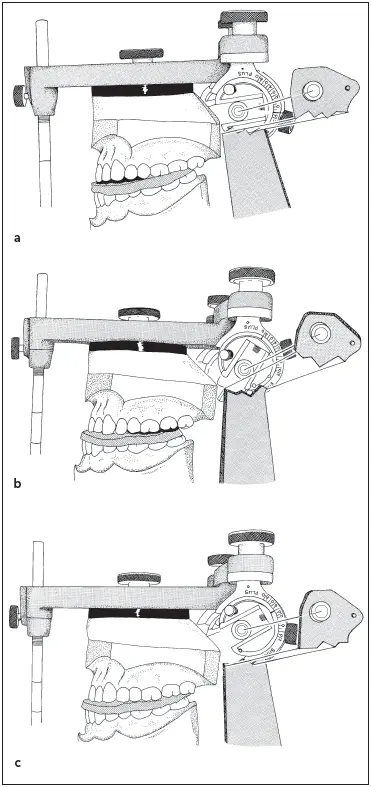
Fig 5-68When using a protrusive interocclusal record to set the condylar guidance, the condylar inclination is rocked up and down. (a) When the angle is too shallow, the anterior teeth lift out of the record. (b) When the inclination is too steep, the posterior teeth lift out. (c) When the cast is completely seated, the inclination is correct.
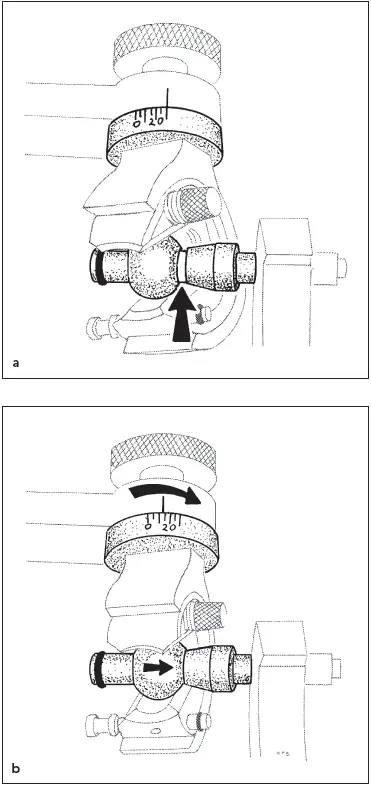
Fig 5-69 (a) With the casts seated in a lateral interocclusal record, there is a gap between the condyle and sleeve. (b) When the Bennett angle ring (and condylar track mechanism) are rotated, the condyle contacts the sleeve. The number on the scale is the angle of the lateral translation.
The condylar inclinations are entered in the patient’s record. The amount of condylar inclination for each condyle is written on the corresponding side of the cast. When teeth are prepared at a future time, it will not be necessary to make new interocclusal records to adjust the articulator. The settings developed during the diagnostic mounting can be reused.
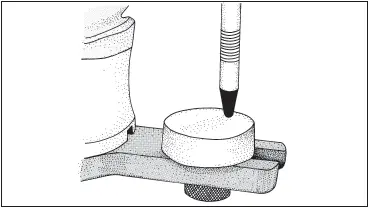
Fig 5-70The incisal guide pin is raised 1.0 mm off the guide block.
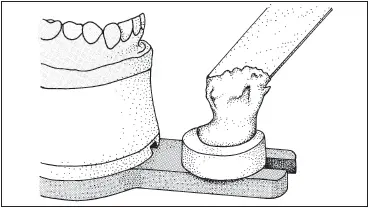
Fig 5-71Tray resin is placed on the incisal block.
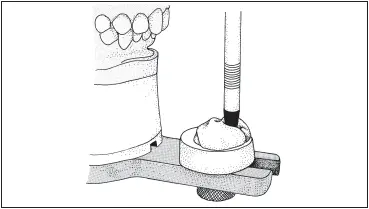
Fig 5-72The guide pin is closed into the soft resin.
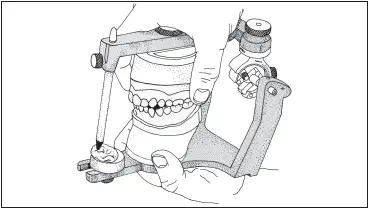
Fig 5-73The casts are moved through all excursions.
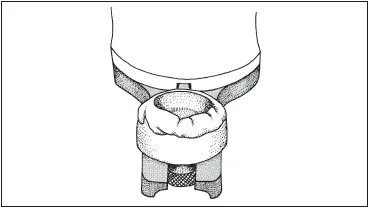
Fig 5-74There is a custom anterior guidance record on the guide block.
Custom anterior guidance
A customized anterior guidance jig can be made for this articulator using a round-end incisal pin and a flat anterior table or an incisal cup. Acrylic resin or a light-cured material (Triad) is molded by the end of the incisal pin in the same manner that the anterior guidance is recorded for the other articulators. The mounted casts are examined on the articulator, and any nonworking interferences are removed. The articulator must be able to move freely with the anterior teeth in contact. If the guidance is inadequate, it is rebuilt to an optimum configuration with a diagnostic wax-up.
The incisal guide pin is raised at least 1 mm off the plastic incisal guide block in all excursions ( Fig 5-70). The surface of the guide block is moistened with monomer. A half scoop of tray resin is mixed, and, while it is still free-flowing, a small amount is placed on the incisal guide. As the polymerizing resin becomes stiffer, more is added until there is about 6 mm (¼ inch) of it covering the guide block ( Fig 5-71). The tip of the incisal guide pin and the occluding surfaces of the anterior teeth are lubricated with petrolatum. The articulator is closed to complete contact between the casts. The guide pin should sink into the soft acrylic resin ( Fig 5-72). The articulator is moved through all excursions repeatedly, keeping the anterior teeth touching at all times ( Fig 5-73). The pathways of all the movements will be imprinted by the tip of the guide pin in the acrylic resin as a permanent record ( Fig 5-74). Movement of the casts is continued until polymerization is complete. The excess is removed.
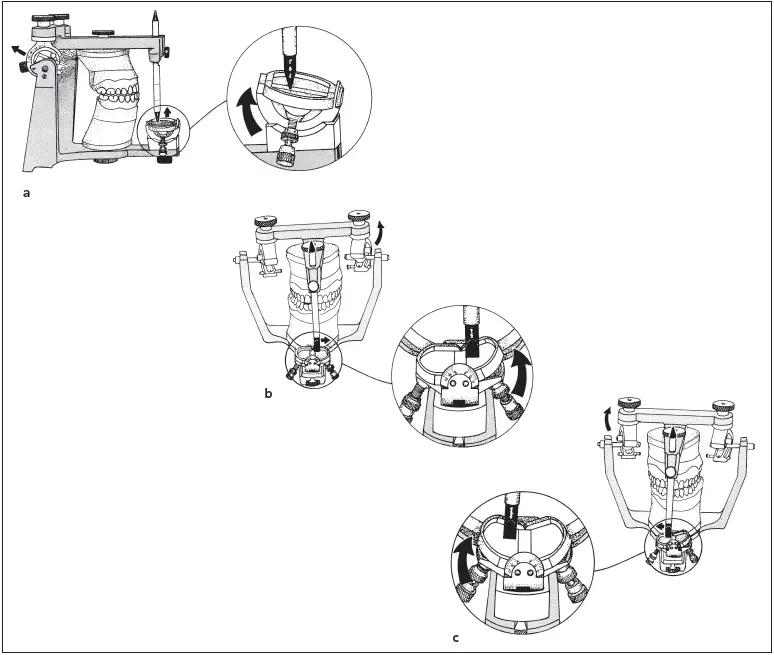
Fig 5-75To set the mechanical incisal guide, the casts are moved into a protrusive relationship. (a) The angulation of the table is increased to contact the pin. (b) The casts are moved into a right lateral excursion, and the left wing of the incisal table is raised. (c) The casts are moved into a left lateral excursion, and the right wing of the table is lifted to complete the recording.
Mechanical anterior guidance
The guidance of mandibular movement imparted by the anterior teeth also can be recorded on this instrument with a mechanical incisal guide. The mounted casts are examined. Any interferences that prevent the anterior teeth from remaining in contact in all excursions are removed from the casts. Any inadequacies in the guidance are restored by building up an optimum configuration in a diagnostic wax-up.
The lock nut under the incisal table at the front end of the lower member of the articulator is loosened. The incisal pin should be in contact with the incisal table.
The casts are protected from undue abrasion by lubrication of the contacting surfaces with petrolatum. The upper member of the articulator is gently moved back to bring the maxillary and mandibular teeth into an end-to-end position. The incisal pin will be lifted off the incisal table. The incisal guide is rotated to raise it posteriorly until it makes contact with the pin ( Fig 5-75a). The lock nut is tightened to maintain this inclination of the table.
The casts are moved into a right lateral excursion. The pin will move to the left side and will again be lifted off the table. The small thumb nut under the left side of the table is loosened, and the elevating screw is used to raise the left wing of the table into contact with the corner of the guide pin ( Fig 5-75b). The process is repeated by moving the casts into a left lateral excursion. The right wing of the incisal table is raised to contact the pin ( Fig 5-75c).
References
1. Pruden WH. The role of study casts in diagnosis and treatment planning. J Prosthet Dent 1960;10:707–710.
2. Hickey JC, Lundeen HC, Bohannan HM. A new articulator for use in teaching and general dentistry. J Prosthet Dent 1967;18:425– 437.
3. Teteruck WR, Lundeen HC. The accuracy of an ear face-bow. J Prosthet Dent 1966;16:1039–1046.
4. Cowan RD, Sanchez RA, Chappell RP, Glaros AG, Hayden WJ. Verifying the reliability of interchanging casts with semiadjustable articulators. Int J Prosthodont 1991;4:258–264.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.