James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Ceramic inlay
Ceramic inlay restorations are used to restore teeth with smallto moderate-sized lesions that permit a narrow preparation isthmus in an area of the mouth where the esthetic demand is high. Premolars should have one intact marginal ridge, but MOD ceramic inlays can be used in molars ( Fig 6-11). This type of restoration can also be etched to enhance bonding, and there is some evidence that the structural integrity of the tooth cusps may be stabilized by bonding. 13The relatively large size of the cavity preparation required for this restoration precludes its use in the treatment of incipient lesions.
Mesio-occlusodistal onlay
This design can be used for restoring moderately large lesions on premolars and molars with intact facial and lingual surfaces ( Fig 6-12). It will accommodate a wide isthmus and up to one missing cusp on a molar. If a cast metal restoration is needed on a premolar with both marginal ridges compromised, it should include occlusal coverage to protect the remaining tooth structure. This restoration also can be considered an extracoronal restoration because of the occlusal coverage that overlays and protects the tooth cusps.
The MOD onlay does not have the necessary resistance to be used as a fixed partial denture retainer. Although ordinarily fabricated of a gold alloy, this restoration design has been used with cast glass and other types of ceramics. Ceramic MOD onlays should be used very cautiously. Without generous occlusal thickness, these restorations are susceptible to fracture.
Extracoronal Restorations
If insufficient coronal tooth structure exists to retain the restoration within the crown of the tooth, an extracoronal restoration, or crown , is needed. It may also be used where there are extensive areas of defective axial tooth structure or if there is a need to modify contours to refine occlusion or improve esthetics.
Partial coverage crown
This is a crown that leaves one or more axial surfaces uncovered ( Fig 6-13). Therefore, it can be used to restore a tooth with one or more intact axial surfaces with half or more of the coronal tooth structure remaining. It will provide moderate retention and can be used as a retainer for short-span fixed partial dentures. If tooth destruction is not excessive, a partial coverage crown with a minimally extended preparation and carefully finished margins can satisfy moderate esthetic demands in the maxillary arch.
All-metal crown
The all-metal conventional crown can be used to restore teeth with multiple defective axial surfaces ( Fig 6-14). It will provide the maximum retention possible in any given situation, but its use must be restricted to situations where there are no esthetic expectations. This will usually limit it to second molars, some mandibular first molars, and occasionally mandibular second premolars. Because less tooth structure must be removed for its preparation than for crowns with a ceramic component, and because its fabrication is the simplest of any crown, this restoration should remain among those designs considered in planning single-tooth restorations on molars as well as posterior fixed partial dentures.
Metal-ceramic crown
A metal-ceramic crown also can be used to restore teeth with multiple defective axial surfaces ( Fig 6-15). It, too, is capable of providing maximum retention, but it also will meet high esthetic requirements. It can be used as a fixed partial denture retainer where full coverage and a good cosmetic result must be combined.
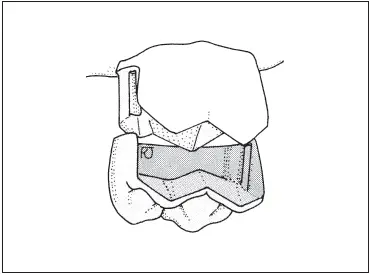
Fig 6-13A three-quarter crown being seated on a molar.
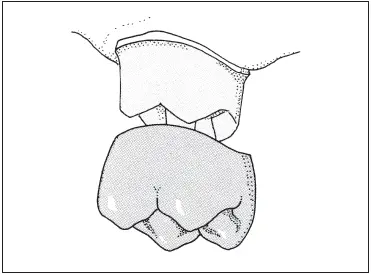
Fig 6-14An all-metal full crown on a maxillary second molar.
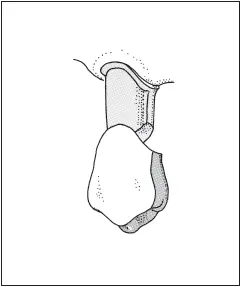
Fig 6-15A metal-ceramic crown on a maxillary premolar.
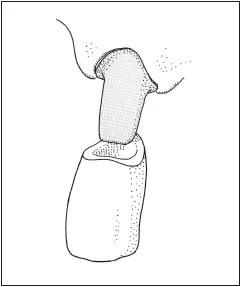
Fig 6-16An all-ceramic crown on an incisor.
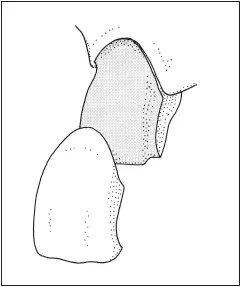
Fig 6-17A ceramic veneer on a maxillary incisor.
All-ceramic crown
When full coverage and maximum esthetics must be combined, an all-ceramic crown is the treatment of choice ( Fig 6-16). All-ceramic crowns are not as resistant to fracture as metal-ceramic crowns, so their use must be restricted to situations likely to produce low to moderate stress. They are usually used for incisors, although cast glass ceramics are also employed in the restoration of posterior teeth. Preparations for this type of restoration on premolars and molars require the removal of large quantities of tooth structure.
Ceramic veneer
Because all-ceramic and metal-ceramic crowns require the removal of such large quantities of tooth structure, there has been considerable interest in less destructive alternatives. The ceramic veneer has emerged as a means of producing an esthetic result on otherwise intact anterior teeth that are marred by severe staining or developmental defects restricted to the facial surface of the tooth ( Fig 6-17). This restoration also can be used to restore moderate incisal chipping and small proximal lesions. The use of a veneer requires only minimal tooth preparation and therefore offers an alternative to crowns that is attractive to the patient and dentist alike.
The features and capabilities of the 12 types of singletooth restorations described in this chapter are shown in Table 6-1.
Table 6-1 Features and applications of single-tooth restorations
Restoration Longevity
Every dentist would like to be able to answer the patient’s question, “How long will my restoration last?” Logical though this question may be, unfortunately it is impossible to answer directly. We cannot predict the life span of a pair of shoes or a television set, and these everyday items are not custom made, nor do they perform their service in a hostile biologic environment, submerged in water.
Clinical studies of restoration longevity have produced widely disparate figures. As a general rule, cast restorations will survive in the mouth longer than amalgam restorations, which in turn will last longer than composite resin restorations. 14A compilation of five studies of 676 patients concluded that amalgam restorations exhibit a 50% failure rate between 5.5 and 11.5 years, with an extrapolated life expectancy of 10 to 14 years. 15
Meeuwissen et al 16reported a 10-year survival rate of 58% for amalgam restorations in Dutch military patients; Arthur et al 17reported an 83% survival rate for the same time span in a US military population. Qvist et al 18found that 50% of the amalgam restorations in a group of Danish patients had failed at 7 years. Christensen 19estimated a 14-year longevity for amalgam restorations. In selected populations, amalgam restorations of unspecified types or sizes in one study14 have shown 10-year survival rates as high as 72%. A 15-year survival rate of 72.8% was reported for simple amalgams in another study. 20
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.