Salivary Gland Pathology
Здесь есть возможность читать онлайн «Salivary Gland Pathology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Salivary Gland Pathology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Salivary Gland Pathology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Salivary Gland Pathology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
now features case presentations to place the information in context, as well as additional treatment algorithms in each chapter to assist in clinical decision making. Written by highly respected clinicians, educators, and researchers with extensive expertise in oral and maxillofacial surgery, this authoritative resource:
Reviews the etiology, diagnosis, and treatment of all salivary gland pathologies, with detailed explanations and hundreds of full-color clinical images Incorporates new information on the taxonomy of salivary gland tumors, neoplastic and non-neoplastic entities, image guided biopsies of salivary gland lesions, and complications in traditional and non-traditional forms of salivary gland surgery Offers expanded coverage of histopathology, including classification, grading, and staging of salivary gland tumors Features up-to-date chapters on anatomy and physiology, imaging, cysts, systemic diseases, tumors, trauma, and innovative salivary gland surgical techniques Includes a discussion of meta-analyses and systematic reviews to support evidence-based practice remains the definitive resource for oral and maxillofacial surgeons, otolaryngologists, head and neck surgeons, and general surgeons as well as their residents providing care for patients with salivary gland pathology.
Salivary Gland Pathology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Salivary Gland Pathology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
These relatively rare tumors exist primarily in the parotid gland. Their imaging characteristics are that of PAs except that they do accumulate 99mTc‐pertechnetate. They are also reported to have high 18F‐FDG uptake. They are considered benign but may have some invasive features.
Malignant Tumors
Mucoepidermoid carcinoma
Mucoepidermoid carcinoma is the most common malignant lesion of the salivary glands. They are also the most common salivary malignancy in the pediatric population. One half occur in the parotid gland and the other half in minor salivary glands (Jansisyanant et al. 2002; Shah 2002). The imaging characteristics of mucoepidermoid carcinoma are based on histologic grade. The low‐grade lesions are sharply marginated and inhomogenous, mimicking PA and Warthin tumor. These well‐differentiated lesions can have increased signal on T2 weighted sequences. The low‐grade lesions are more commonly cystic (Madani and Beale 2006b). The high‐grade, invasive lesions mimic adenoid cystic carcinoma and lymphoma or large heterogeneous PAs or carcinoma ex‐pleomorphic adenoma. They tend to have a lower signal of T2. Contrast‐enhanced studies demonstrate enhancement in the more solid components (Sigal et al. 1992; Lowe et al. 2001; Bialek et al. 2006; Madani and Beale 2006b) ( Figures 2.64through 2.66). Therefore, standard imaging cannot exclude a malignant neoplasm. Defining the tumor's extent is critical. Contrast MRI, especially in the coronal or sagittal plane, is essential to identify perineural invasion into the skull base.
Adenoid cystic carcinoma
Adenoid cystic carcinoma has similar characteristics as mucoepidermoid carcinoma in that their imaging findings are based on histologic grade. Adenoid cystic carcinoma is the most common malignant neoplasm of the submandibular and sublingual glands as well as the minor salivary glands in the palate. These tumors have a high rate of local recurrence, higher rate of distance metastases as opposed to nodal disease, and may recur after a long latency period (Madani and Beale 2006b). MRI is the imaging method of choice, demonstrating high signal due to increased water content. Contrast‐enhanced fat saturated images are critical to evaluate for perineural spread, which is demonstrated by nerve thickening and enhancement (Madani and Beale 2006b; Shah 2002). CT can be helpful to evaluate bone destruction or foraminal widening. It is important to define the tumors' extent and identify perineural invasion into the skull base ( Figures 2.67through 2.71).

Figure 2.64. Axial contrast‐enhanced CT demonstrating an ill‐defined mass diagnosed as a mucoepidermoid carcinoma (arrow).
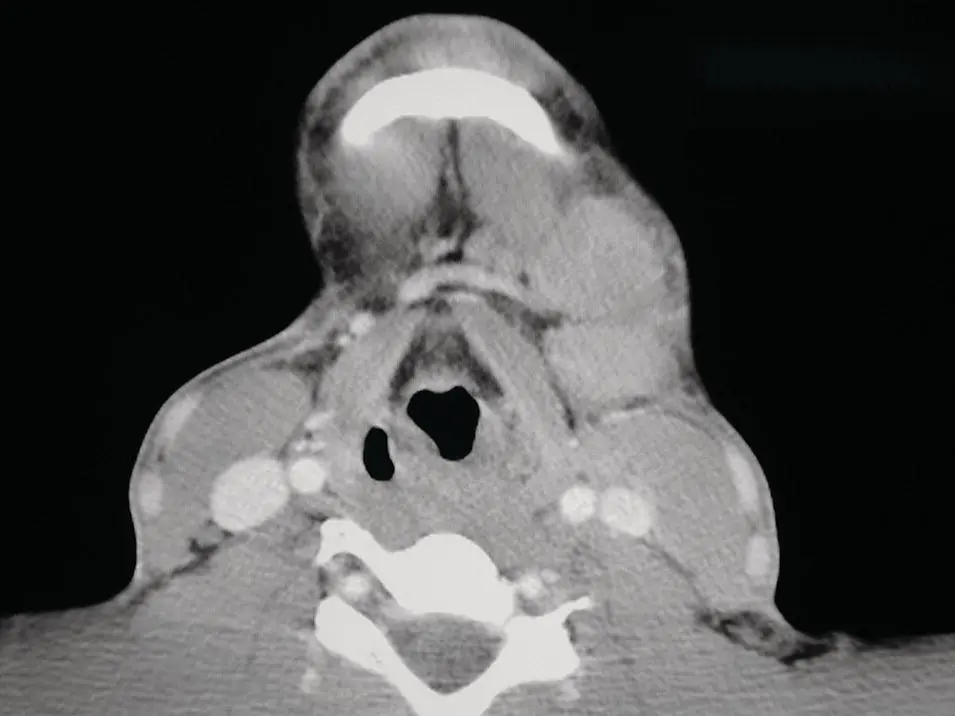
Figure 2.65.Axial contrast‐enhanced CT demonstrating large bulky cervical lymphadenopathy with ill‐defined borders, diagnosed as a mucoepidermoid carcinoma.
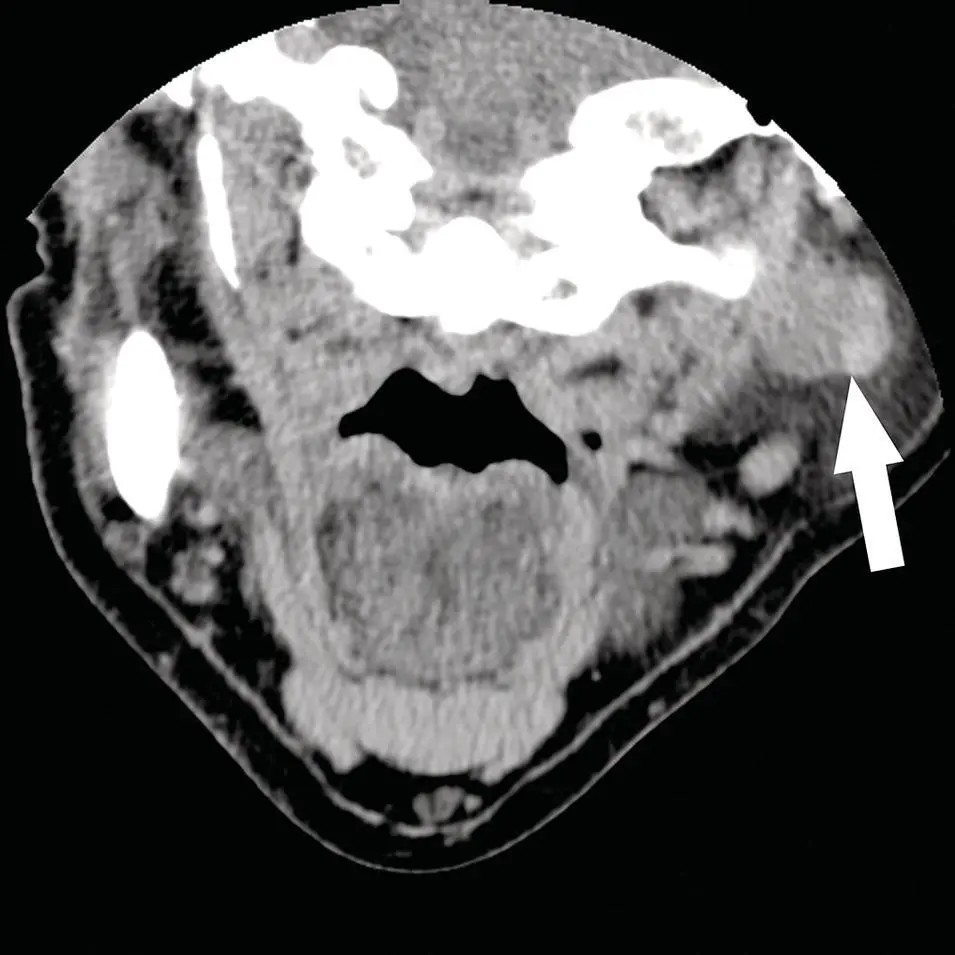
Figure 2.66. Reformatted coronal contrast‐enhanced CT demonstrating an ill‐defined heterogeneous density mass diagnosed as a mucoepidermoid carcinoma (arrow).

Figure 2.67. Coronal contrast‐enhanced MRI of the skull base demonstrating a mass extending through the skull base via the left foramen ovale (arrow), diagnosed as an adenoid cystic carcinoma originating from a minor salivary gland of the pharyngeal mucosa.
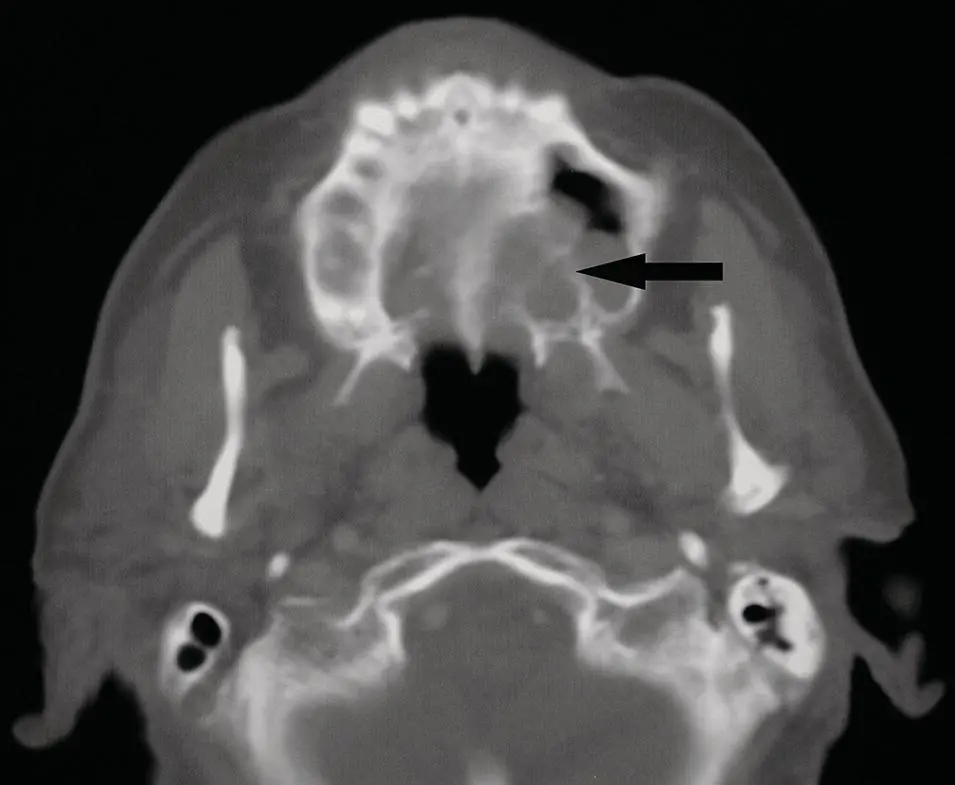
Figure 2.68. Axial CT in bone window demonstrating a mass eroding through the left side of the hard palate and extending into the maxillary sinus (arrow) diagnosed as adenoid cystic carcinoma.
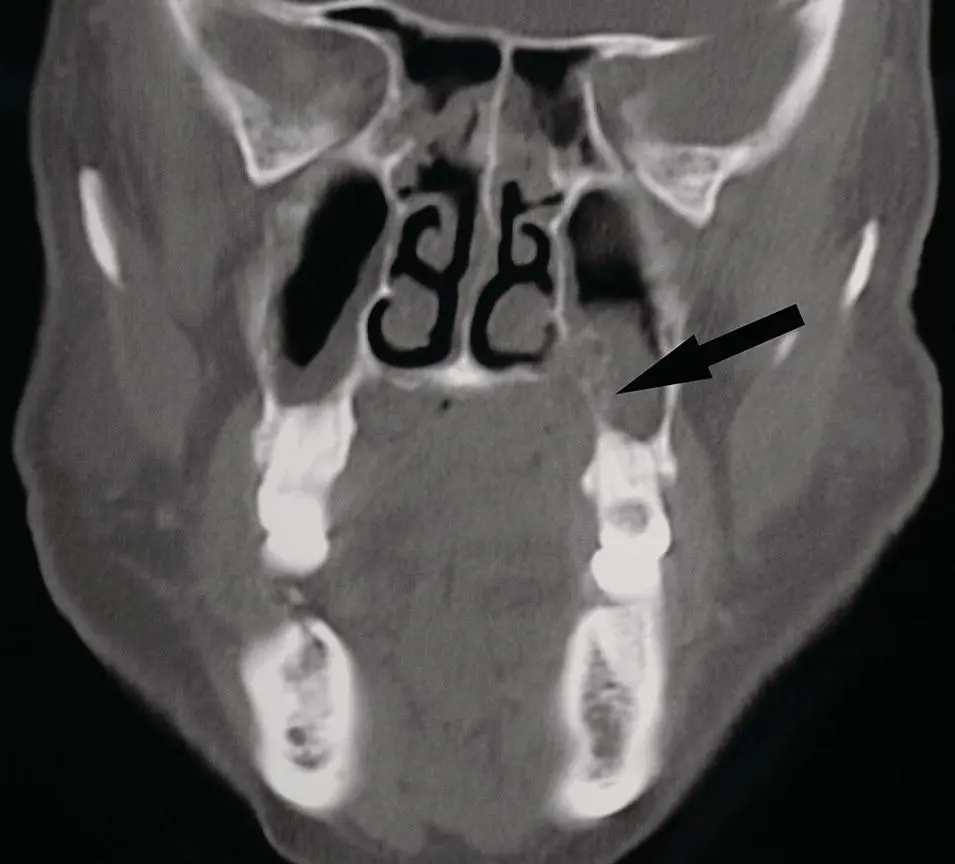
Figure 2.69.Coronal CT corresponding to the case illustrated in Figure 2.68with a mass eroding the hard palate and extending into the left maxillary sinus (arrow).
NEOPLASMS – NON‐SALIVARY
Benign
Lipoma
In the cervical soft tissues, lipomas are slightly more commonly seen within the parotid gland rather than periparotid. Lipomas of the salivary glands are uncommon (Shah 2002). The CT and MRI characteristics are those of subcutaneous fat with CT density very low (approximately 100 H) and hyperintense on both T1 and T2. Lipomas tend to be echogenic on US. They may be uniform on imaging but may have areas of fibrosis. The heterogenous density from fibrosis, or hemorrhage, carries the additional differential diagnosis of liposarcoma or other neoplasms (Som et al. 1995), ( Figures 2.72and 2.73).

Figure 2.70.Reformatted contrast‐enhanced coronal CT with a mass in the right submandibular gland (arrow) diagnosed as an adenoid cystic carcinoma.
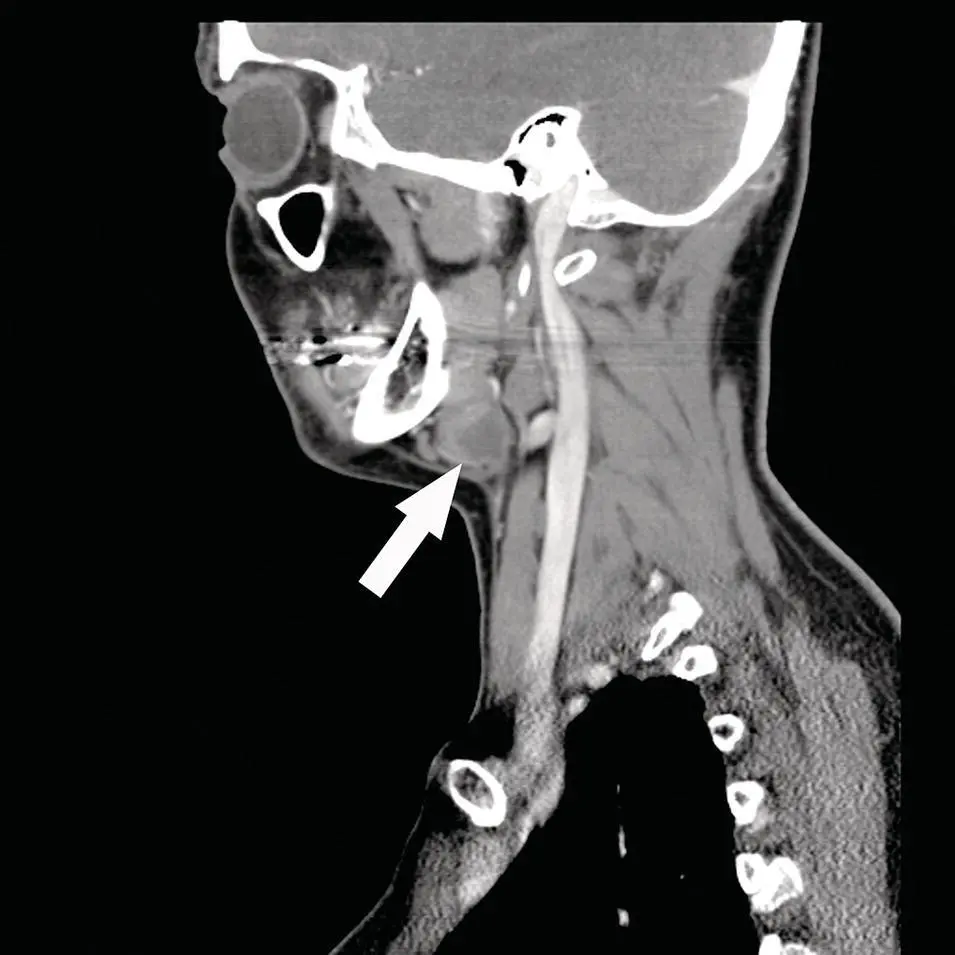
Figure 2.71. Reformatted sagittal contrast‐enhanced CT corresponding to the case illustrated in Figure 2.65.

Figure 2.72. Axial contrasted‐enhanced CT of the head with a fat density mass at the level of the parotid gland and extending to the submandibular gland, diagnosed as a lipoma.
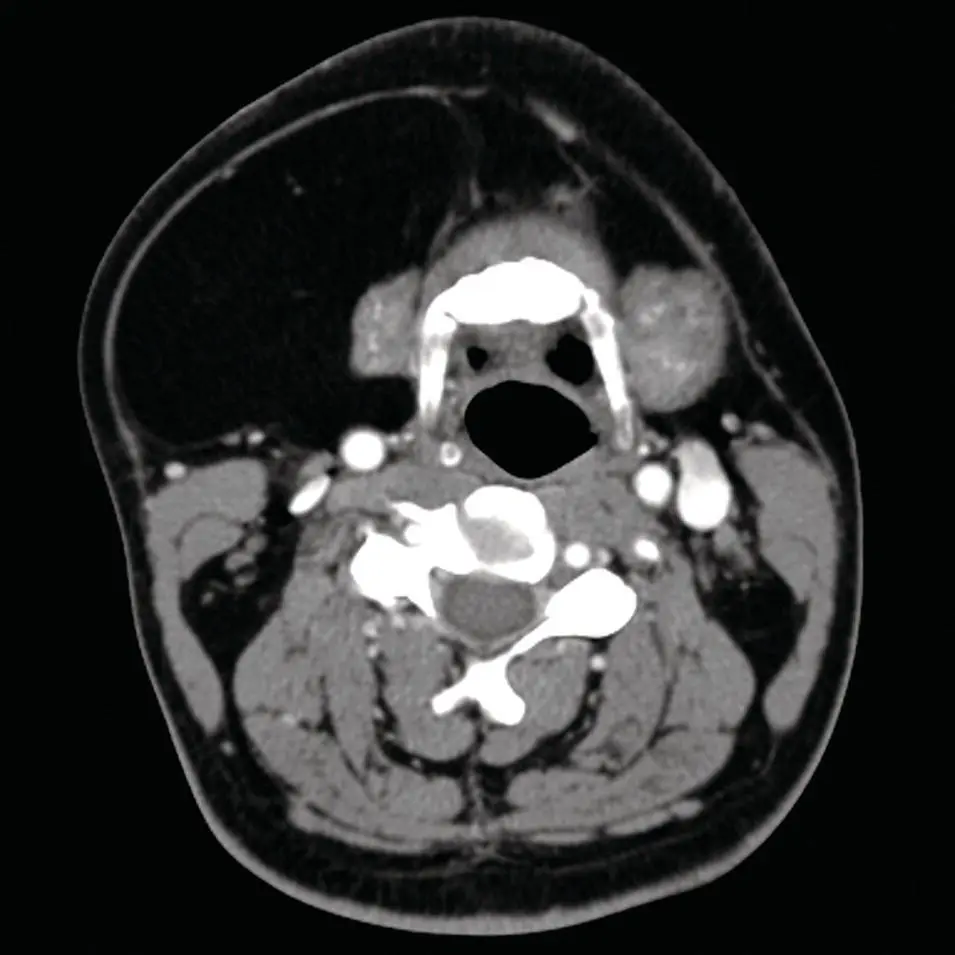
Figure 2.73. Axial contrast‐enhanced CT through the submandibular gland with fat density mass partially surrounding the gland. A lipoma was diagnosed.
Neurogenic tumors
Neurogenic tumors are uncommon in the salivary glands but when encountered are most commonly found in the parotid gland. Most facial nerve schwannomas are on the intratemporal facial nerve with only 9% extra‐temporal and in the parotid gland (Shimizu et al. 2005), ( Figures 2.74through 2.76). These are difficult to preoperatively diagnose as they do not typically present with facial nerve dysfunction. As seen in other parts of the body, they tend to be sharply marginated and have an ovoid shape along the axis of the involved nerve, such as the facial nerve. The CT density is that of soft tissue but post‐contrast, both enhance (schwannoma slightly greater than neurofibroma). Both are noted as low signal on T1 and high on T2. MRI enhancement pattern follows that of CT. They may demonstrate a target sign appearance with peripheral hyperintensity relative to a central hypointensity (Martin et al. 1992; Suh et al. 1992; Shimizu et al. 2005). However, this sign is not pathognomonic and may be seen in schwannomas or neurofibromas. Increased uptake is seen on FDG PET in both diseases. The neurofibroma may be associated with Von Recklinghausen's disease. Although, most schwannomas and neurofibromas are benign, they are reported as demonstrating increased uptake (hypermetabolism of glucose) of 18F‐FDG on PET imaging (Hsu et al. 2003). Although the calculated standard uptake value (SUV) can be helpful in differentiating benign from malignant lesions, there is a significant overlap (Ioannidis and Lau 2003). There is difficulty in separating low‐grade malignant lesions from benign lesions (Ioannidis and Lau 2003), ( Figures 2.77and 2.78). Plexiform neurofibromas are also slow‐growing and rare. They present with multiple cord‐like masses and are far more common in the parotid gland relative to other salivary glands. By CT and MRI, they are sometimes described as a “branching” pattern or “bag of worms” secondary to the multiple lesions growing along nerve branches. They have CT and MRI signal characteristics like neurofibromas and schwannomas including the “target sign” (Lin and Martel 2001; Aribandi et al. 2006). The target sign may also be seen by US as a hypoechoic periphery surrounding a subtle and slightly hyperechoic center. There may also be slight increase through‐transmission (Lin and Martel 2001).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Salivary Gland Pathology»
Представляем Вашему вниманию похожие книги на «Salivary Gland Pathology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Salivary Gland Pathology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.