Salivary Gland Pathology
Здесь есть возможность читать онлайн «Salivary Gland Pathology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Salivary Gland Pathology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Salivary Gland Pathology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Salivary Gland Pathology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
now features case presentations to place the information in context, as well as additional treatment algorithms in each chapter to assist in clinical decision making. Written by highly respected clinicians, educators, and researchers with extensive expertise in oral and maxillofacial surgery, this authoritative resource:
Reviews the etiology, diagnosis, and treatment of all salivary gland pathologies, with detailed explanations and hundreds of full-color clinical images Incorporates new information on the taxonomy of salivary gland tumors, neoplastic and non-neoplastic entities, image guided biopsies of salivary gland lesions, and complications in traditional and non-traditional forms of salivary gland surgery Offers expanded coverage of histopathology, including classification, grading, and staging of salivary gland tumors Features up-to-date chapters on anatomy and physiology, imaging, cysts, systemic diseases, tumors, trauma, and innovative salivary gland surgical techniques Includes a discussion of meta-analyses and systematic reviews to support evidence-based practice remains the definitive resource for oral and maxillofacial surgeons, otolaryngologists, head and neck surgeons, and general surgeons as well as their residents providing care for patients with salivary gland pathology.
Salivary Gland Pathology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Salivary Gland Pathology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
ACUTE SIALADENITIS
Acute sialadenitis may be bacterial or viral in nature and may be a result of obstruction from a calculus, stricture or mass (see Chapters 3and 5). Viral parotitis or mumps may be caused by a variety of viruses but most commonly the paromyxovirus is the culprit. The patient presents with an enlarged, tender, and painful gland. Acute suppurative parotitis (sialadenitis) presents in a similar manner as viral parotitis with the additional sign of purulent exudate. Oral bacterial pathogens are the causative agents, with staphylococcal and streptococcal species being the most common. CT scan demonstrates an enlarged gland with ill‐defined margins and infiltration of the surrounding fat by edema fluid. The gland, especially the parotid, is increased in density because of the edema fluid, which is of higher density than fat. CT contrast demonstrates heterogenous enhancement and may show an abscess. On T1 MRI scan, the overall gland signal may be decreased slightly from the edema but does enhance heterogeneously with contrast. T2 MRI scan shows increased signal secondary to edema. Both CT and MRI may demonstrate enhancement and enlargement of the parotid (or sublingual) duct. US shows slight decrease in echogenicity relative to normal. These patterns are not unique to bacterial or viral infection or inflammation and may be seen with autoimmune diseases such as Sjögren syndrome or a diffusely infiltrating mass. The surrounding subcutaneous fat also demonstrates heterogenous increased density from edema, resulting in a “dirty fat” appearance. There is also thickening of fascia and the platysma muscle (Shah 2002; Bialek et al. 2006; Madani and Beale 2006a).
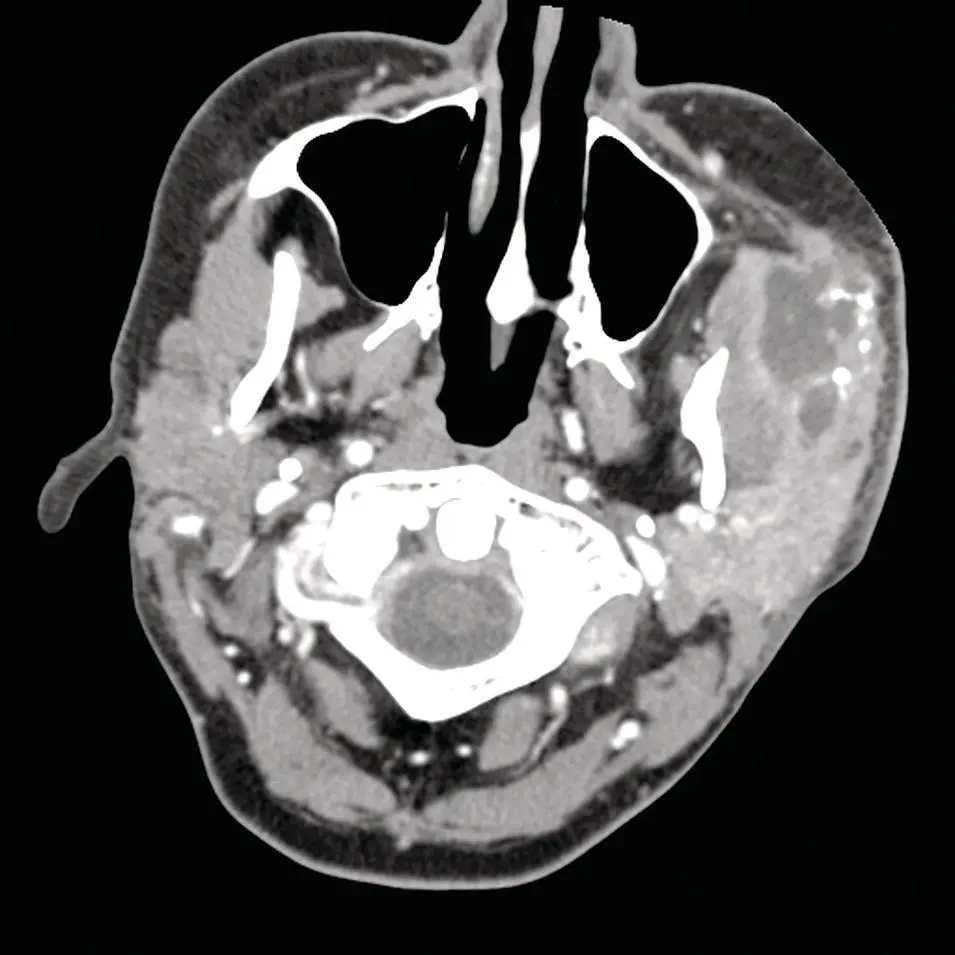
Figure 2.52. Axial CT with contrast at the level of the masseter muscles demonstrating a left accessory parotid gland abscess.
With acute submandibular sialadenitis, the gland becomes enlarged and may be associated with a dilated duct if a sialolith is present. By CT, the calculus may be readily identified but not as easily seen by MRI. There may be varying degrees of cellulitis or frank abscess formation. The inflamed gland undergoes greater contrast enhancement. MRI demonstrates an enlarged heterogenous gland with dilated fluid‐filled duct and gland which on T2 images is of high signal. On ultrasound, the acutely inflamed gland demonstrates enlargement with focal hypoechoic foci (Shah 2002; Bialek et al. 2006; Madani and Beale 2006a), ( Figures 2.52through 2.54).
CHRONIC SIALADENITIS
The etiology of chronic inflammatory states of the salivary glands varies by the specific gland in question. Chronic inflammatory changes in the parotid gland tend to be related to autoimmune disease (Sjögren syndrome), recurrent suppurative parotitis, or radiation injury. Other etiologies include granulomatous infections such as tuberculosis or sarcoidosis. Chronic inflammation of the submandibular gland and, to a lesser degree, the sublingual gland is more commonly due to obstructive disease, particularly sialolithiasis. In the chronically inflamed state, the glands are enlarged but over longer periods of time progressively reduced in size, and heterogenous density may be seen on CT with extensive fibrosis and small focal (punctate) calcification. The density on CT is often increased due to cellular infiltration and edema during acute phases of exacerbation. The surrounding subcutaneous fat may not show signs of edema as is seen with acute sialadenitis. MRI demonstrates similar changes with heterogenous signal on both T1 and T2. The duct or ducts may be dilated, strictured, or both. Both may be visible by contrast CT and MRI (Sumi et al. 1999b; Shah 2002; Bialek et al. 2006; Madani and Beale 2006a). Chronic sclerosing sialadenitis (aka Kuttner tumor, or IgG4‐related disease [see Chapter 6]) can mimic a mass of the salivary (most commonly submandibular) glands (Huang et al. 2002). It presents with a firm, enlarged gland mimicking a tumor. The most common etiology is sialolithiasis (50–83%) but other etiologies include chronic inflammation from autoimmune disease (Sjögren syndrome), congenital ductal dilatation and stasis, disorders of secretion (Huang et al. 2002). It is best diagnosed by gland removal and pathologic examination as fine needle aspiration biopsy may be misleading (Huang et al. 2002). Chronic sialadenitis can also be caused by chronic radiation injury. US studies have demonstrated a difference in imaging characteristics between submandibular sialadenitis caused by acalculus versus calculus disease. The acalculus sialadenitis submandibular gland US demonstrates multiple hypoechoic lesions, mimicking cysts, with diffuse distribution throughout a heterogenous hypoechoic gland. They did not, however, demonstrate increased thru transmission, which is typically seen with cysts and some soft‐tissue tumors. Sialadenitis caused by calculus disease demonstrates hyperechoic glands relative to the adjacent digastric muscle, but some are iso‐ or hypoechoic relative to the contralateral gland (Ching et al. 2001).
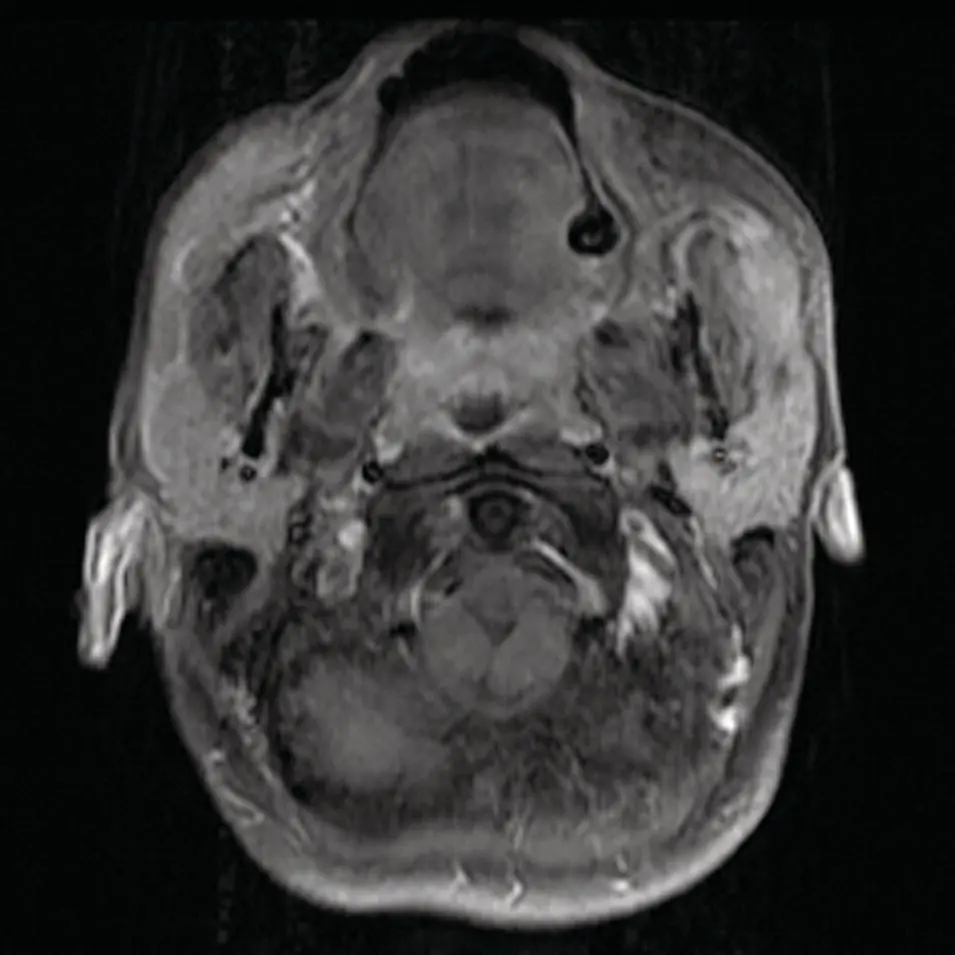
Figure 2.53.Axial contrast‐enhanced fat saturated T1 MRI demonstrating heterogenous enhancement consistent with abscess of the left accessory parotid gland.
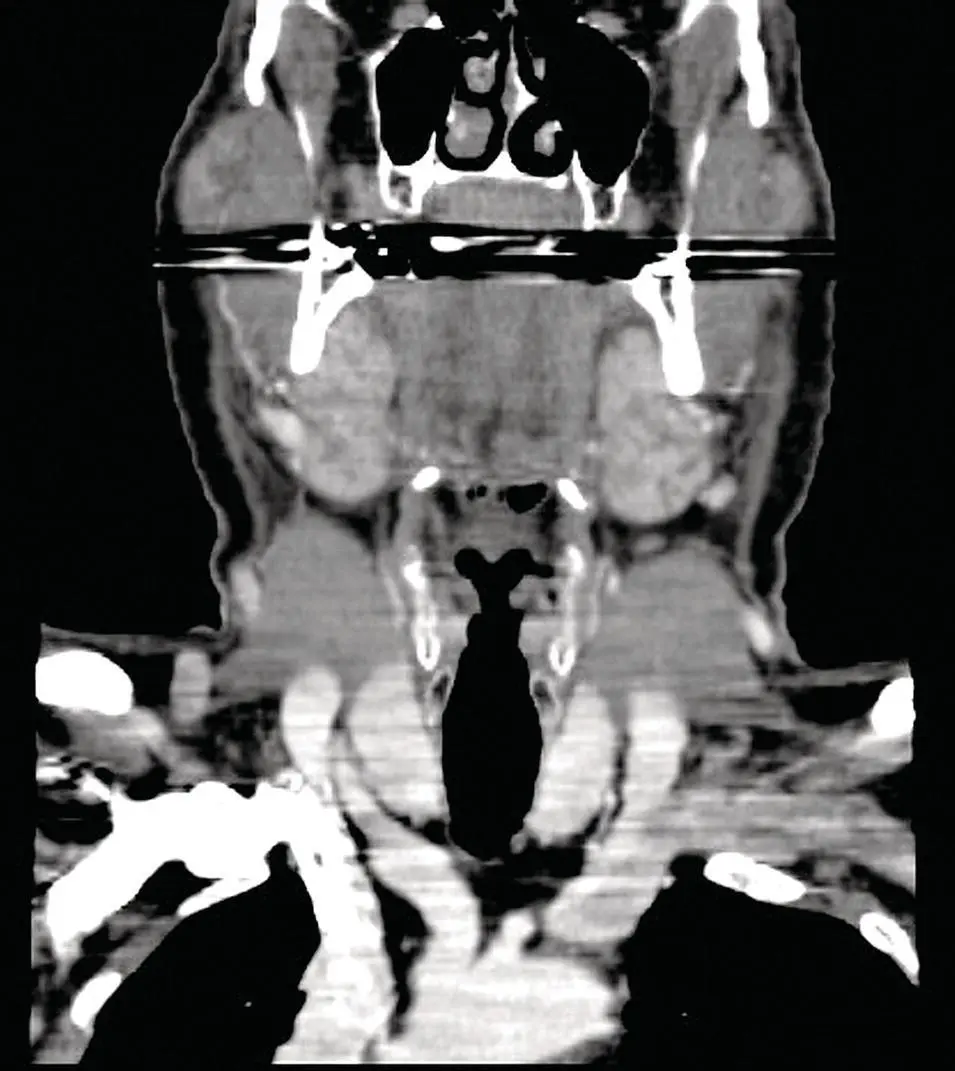
Figure 2.54. Reformatted coronal CT demonstrating enlargement and enhancement of the submandibular glands consistent with viral sialadenitis.
HIV‐ASSOCIATED LYMPHOEPITHELIAL LESIONS
These lesions are comprised of mixed cystic and solid masses within the parotid (much less in the SMG and SLG). CT shows multiple cystic and solid masses with associated parotid enlargement. IV contrast shows mild peripheral enhancement in the cysts and more heterogenous enhancement in the solid lesions ( Figure 2.55). MRI images of the cysts are typical with low signal on T1 and high on T2. The more solid lesions are of heterogenous soft‐tissue signal on T1 and increase on T2. Contrast MRI images follow the same pattern as CT (Holliday 1998). The US images show heterogenous cystic lesions with internal architecture of septation and vascularity and slightly hypoechoic signal of the solid masses. Mural nodules may be seen in predominantly cystic lesion. Associated cervical lymphadenopathy is commonly seen as well as hypertrophy of tonsillar tissues. Differential diagnosis of these findings includes Sjögren syndrome, lymphoma, sarcoidosis, other granulomatous diseases, metastases, and Warthin tumor (Kirshenbaum et al. 1991; Som et al. 1995; Martinoli et al. 1995; Shah 2002; Madani and Beale 2006a).
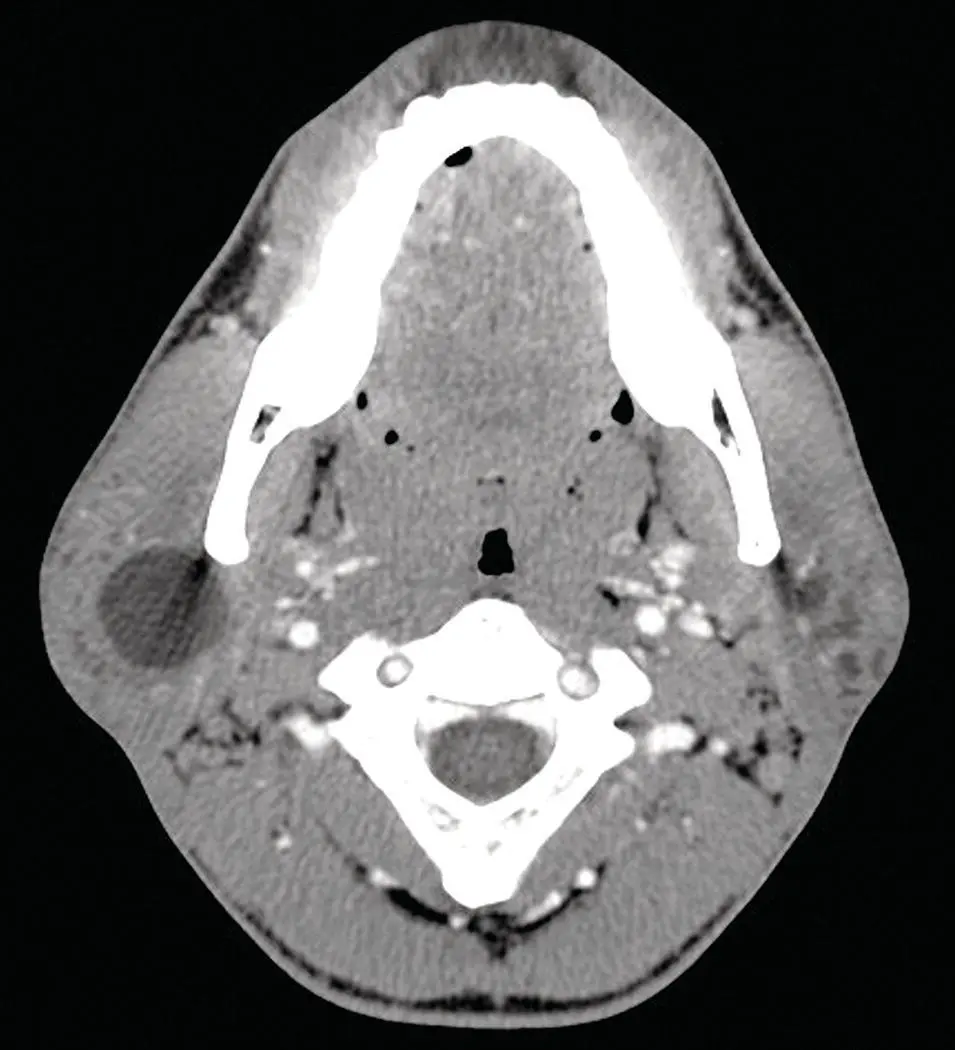
Figure 2.55. Axial CT demonstrating a large cystic lesion in the right parotid gland and multiple small lesions in the left parotid diagnosed as lymphoepithelial cysts.
MUCOUS ESCAPE PHENOMENA
The mucous escape phenomenon most commonly results from obstruction in the sublingual gland, resulting in a backup of salivary secretions (see Chapter 4). Ductal obstruction may be caused by calculi, stricture from prior infection or trauma. The chronic dilatation of the duct and accumulation of fluid produces a cystic mass by CT, MRI, and US. The simple ranula remains in the sublingual space and typically presents with a unilocular, well‐demarcated and homogenous structure unless complicated by hemorrhage or infection. The walls may enhance slightly if a ranula remains contained above the mylohyoid muscle. It may rupture into the surrounding tissues and extravasate along a path of least resistance and extend inferiorly into the submandibular space or posteriorly into the parapharyngeal space under which circumstances it is termed a plunging ranula (see Chapter 4). The non‐plunging ranula has a dilated ovoid configuration on axial images, but when it herniates into the submandibular space the dilated space shrinks into a tail‐like configuration in the sublingual space. The tail sign is pathognomonic for ranulae and may be seen in both simple and plunging types. The ranula can usually be differentiated from a hemangioma and lymphangioma by its lack of internal architecture (unless complicated). The ranulas are typically homogenous internally with well‐defined margins, unless infected or hemorrhagic, follow fluid density on CT (isodense to simple fluid) and intensity on MRI (low on T1 and high on T2). Both simple and plunging ranulae have these characteristics. The plunging component may be in the parapharyngeal space if the lesion plunges posterior to the mylohyoid muscle or in the anterior submandibular space if it plunges through the anterior and posterior portions of the mylohyoid muscle or through a defect in the muscle. Involvement of the parapharyngeal space and the submandibular space results in a large cystic mass termed “giant ranula” and may mimic a cystic hygroma (Cholankeril and Scioscia 1993; Kurabayashi et al. 2000; Macdonald et al. 2003; Makariou et al. 2003).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Salivary Gland Pathology»
Представляем Вашему вниманию похожие книги на «Salivary Gland Pathology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Salivary Gland Pathology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.