Sheila Annie Peters - Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations
Здесь есть возможность читать онлайн «Sheila Annie Peters - Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The first book dedicated to the emerging field of physiologically based pharmacokinetic modeling (PBPK) Physiologically Based Pharmacokinetic (PBPK) Modelling and Simulations: Principles, Methods, and Applications in the Pharma Industry
Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations: Principles, Methods, and Applications in the Pharmaceutical Industry, Second Edition
Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
TABLE 1.5. Classes of Pharmacological Targets
| Pharmacological Target Class | Examples of Targets | Location | Endogenous Ligands | Type of Drug |
|---|---|---|---|---|
| G‐protein‐coupled receptors (GPCRs) | Adrenoreceptor, metabotropic neurotransmitter receptors (metabotropic glutamate receptors or mGluRs, muscarinic acetylcholine receptors, GABA‐B receptor, 5HT1, 5HT2), CCR, opioid, NK | Transmembrane, cell surface or intracellular | Neurotransmitters a and hormones b | Competitive, noncompetitive, and irreversible antagonist, agonists, partial agonist, or inverse agonist. |
| Receptor tyrosine kinase | EGF, VEGF, PDGF, FGF, HGF, TIE, Trk, MuSK, RYK, and insulin receptor families | Cell surface | Growth factors, c insulin | Competitive, noncompetitive, and irreversible antagonist, agonists, partial agonist, or inverse agonist. |
| Guanylyl cyclase receptors | GC‐A, GC‐B, GC‐C | Cell surface | Guanosine‐5′‐triphosphate (GTP) | Competitive, noncompetitive, and irreversible antagonist, agonists, partial agonist, or inverse agonist. |
| Nuclear receptors | Thyroid hormone‐like, estrogen‐like, glucocorticoid receptors, PPAR, FXR, LXR, and other orphan receptors | Cytosol or translocated to nucleus | Retinoic acid, vitamin D 3, hormones | Competitive, noncompetitive, and irreversible antagonist, agonists, partial agonist, or inverse agonist. |
| Ligand‐gated ion channels or ionotropic receptors | Glutamate cationic receptor, nicotinicoid receptor (5‐HT3, nicotinic acetylcholine receptor, GABA‐A) | Synapses | Neurotransmitters | Competitive, noncompetitive, and irreversible antagonist, agonists, partial agonist, or inverse agonist. |
| Voltage‐gated ion channels | NaV, KV, and CaV | Transmembrane ion channels found along the axon and at the synapse in neurons and in other cells | Respond to changes in voltage | Blocker, inhibitor |
| Enzymes and factors | Transferases such as RNA directed DNA‐polymerase; oxidoreductases such as HMG‐CoA reductase and cyclooxygenases | Cell surface, intracellular, or membrane spanning | Large variety of endogenous and exogenous substrates | Inhibitor activator |
| Peptidases such as ACE, trypsin, thrombin, clotting factors, renin, HIV protease, cathepsin, and caspase | ||||
| Structural proteins | α,β,γ,δ, and ε tubulin | Extracellular or intracellular | GTP | Inhibitor |
a Neurotransmitters are amino acids such as glutamate, aspartate, serine, GABA, and glycine; monoamines such as dopamine, 5‐HT, adrenaline, noradrenaline, and melatonin; neuropeptides; acetylcholine, adenosine, histamine, anadamide, etc.
b Hormones could be derivatives of the amino acids tyrosine and tryptophan. Examples are catecholamines and thyroxine. Peptide hormones consist of chains of amino acids. Examples are TRH and vasopressin. Examples of protein hormones include insulin and growth hormone. More complex protein hormones bear carbohydrate side chains and are called glycoprotein hormones. Luteinizing hormone, follicle‐stimulating hormone, and thyroid‐stimulating hormone are examples of glycoprotein hormones. Lipid and phospholipid‐derived hormones are derivatives of lipids such as linoleic acid and arachidonic acid and phospholipids. Steroid hormones are derived from cholesterol and eicosanoids. Examples of steroid hormones are testosterone and cortisol. Sterol hormones such as calcitriol are a homologous system. The adrenal cortex and the gonads are primary sources of steroid hormones. Examples of eicosanoids are the widely studied prostaglandins.
c Growth factors: Fibroblast growth factors comprise the largest family of growth factor ligands at 23 members. The natural alternate splicing of four fibroblast growth factor receptor (FGFR) genes results in the production of over 48 different isoforms of FGFR. Vascular endothelial growth factor (VEGF) is one of the main inducers of endothelial cell proliferation and permeability of blood vessels; The platelet‐derived growth factors PDGF‐A and ‐B have been recognized as important factors regulating cell proliferation, cellular differentiation, cell growth, development, and many diseases including cancer. Neurotrophins are critical to the functioning of the nervous system. Angiopoietins are protein growth factors required for the formation of blood vessels (angiogenesis). Others include epidermal growth factor (EGF) and hepatocyte growth factor (HGF).
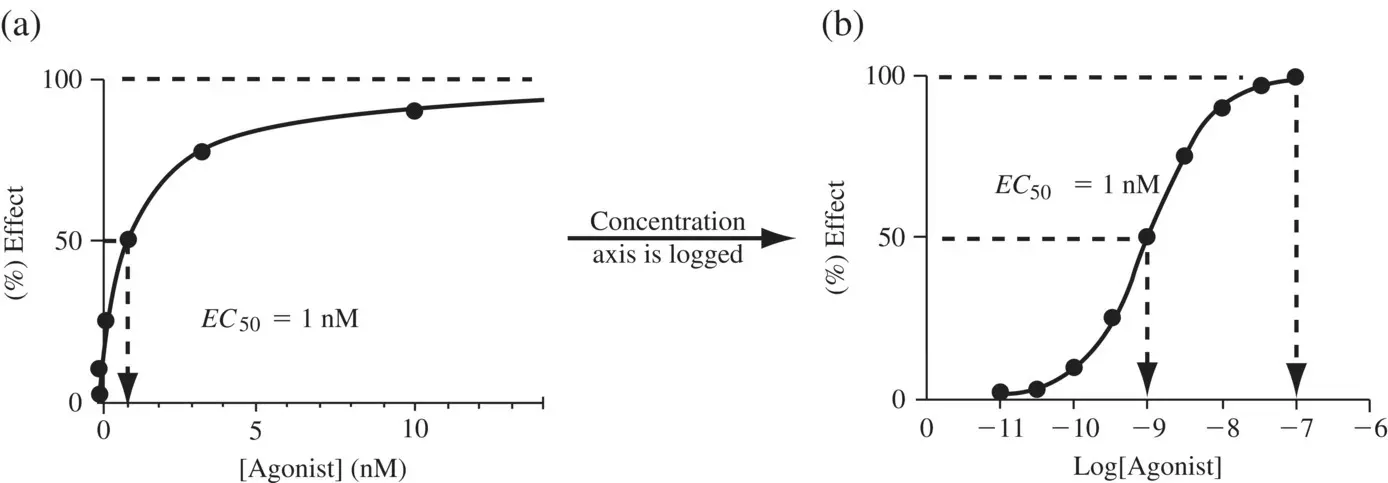
Figure 1.12. Concentration–response curve of an agonist in (a) linear (b) log scale.
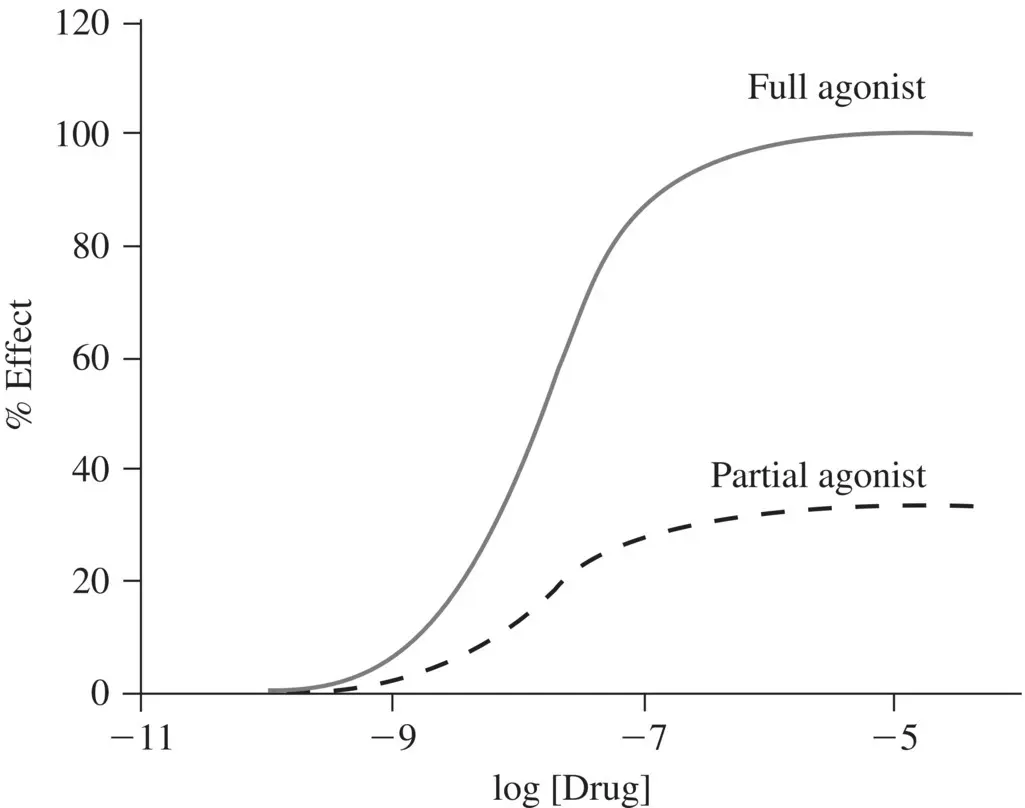
Figure 1.13. Concentration–response curves of a partial agonist and a full agonist both of which have a similar affinity towards the receptor.
Small molecule drugs are selective rather than specific, which means that they rarely produce a single effect. Even if a drug were to act on a single receptor, this receptor may be ubiquitously expressed and may be present in organs where the drug is not intended to act. Alternatively, the targeted receptor may exist in other isoforms which, when affected, can produce adverse effects. Additionally, drugs may act on several receptor classes. A primary effect is the desired therapeutic effect. Secondary effects include all other effects besides the desired effect and may be either beneficial (which is rare) or harmful. With appropriately designed PK and PD studies, one can potentially interpret and predict the outcome of primary and secondary effects. PD involves a study of the relationships between plasma drug concentrations, receptor occupancy, receptor activation and the pharmacological effect, aided by the biochemical and physiological mechanisms of drug action. For drugs which have low membrane permeability or which are substrates of drug transporters, target tissue concentrations rather than plasma concentrations should correlate well with the observed pharmacological effect.
1.5.2 Functional Adaptation Processes
One of the perils of drug development is the occurrence of time‐dependent modulations in pharmacological activity upon repeat administration of certain drugs, arising from functional adaptation processes such as desensitization and sensitization .
1.5.2.1 Desensitization, Tolerance, and Tachyphylaxis
Receptor‐mediated responses to drugs often desensitize with time. This reduced response to an agonist, which is usually reversible upon cessation of treatment, is called desensitization. A second exposure to the agonist after a lapse usually restores response. Agonists that desensitize receptors due to conditioning mechanisms can trigger tolerance and addiction. Some examples of addictive medicines are tranquilizers and sedatives (sleeping pills). Many of these belong to a group of similar substances called benzodiazepines, which allosterically potentiate GABA type A receptor (Sieghart, 1994). Desensitization is often used to suggest a reduced response by any mechanism – receptor phosphorylation, uncoupling, antagonistic metabolites, or negative physiological feedback that occurs over a relatively short period of time, while tolerance is reserved for reduced responsiveness developing over longer periods, usually because of receptor downregulation. Tachyphylaxis is a rapidly developing desensitization after just one or two administrations of the drug.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations»
Представляем Вашему вниманию похожие книги на «Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.