Mount Sinai Expert Guides
Здесь есть возможность читать онлайн «Mount Sinai Expert Guides» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Mount Sinai Expert Guides
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Mount Sinai Expert Guides: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Mount Sinai Expert Guides»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Mount Sinai Expert Guides — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Mount Sinai Expert Guides», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Advance the needle while pulling on the syringe filled with 1% lidocaine and epinephrine. When air is drawn into the syringe you have entered the trachea.Aspiration of air confirms intraluminal tracheal placement. Entering the ET is a possibility; however it would require an extraordinary effort in piercing during the needle insertion. More likely you are in the trachea where the needle tip may be scratching the ET surface. The cuff may be ruptured at this point, but you should simply proceed. Adding to the tidal volume earlier should maintain ventilation.Immediately ‘anchor’ the needle by placing your fingers at the junction of the needle and the skin of the neck to avoid dislodgment. Inject 5 mL of the 1% lidocaine/epinephrine solution.Repeatedly reaffirm placement by demonstrating air bubbles during the procedure, especially if there is dislodgment from movement or otherwise. At any time if the location of needle is of concern start the procedure again, including palpating the trachea as above.
Once the needle is touching the ET, the respiratory therapist pulls the ET back and forth which leads to tugging the needle in your fingers and affirming your position on the ET ( Figure 6.3A).The ET is then gradually pulled to the 20 cm mark or when you no longer feel the ET any more ( Figure 6.3B), usually between 18 and 19 cm.
Angle the needle caudally and pass the catheter. It should pass easily into the trachea.If there is immediate resistance to advancing the catheter, you may not be in front of the ET, or possibly in a blind pouch. Return the needle to the perpendicular position; reaffirm position with air bubbles and have the respiratory therapist pull the ET slightly further cephalad. Retry passing the catheter as above.The guidewire is now advanced into the trachea and should pass freely, inducing a cough when at the bifurcation. At this point, bronchoscopic or US confirmation can be performed ( Figure 6.4).
Using the scalpel, make a perpendicular cut longitudinally, next to the guidewire, above and below it. The single straight dilator follows, opening the tracheotomy, after which blood‐tinged secretions may be seen bubbling through the incision. The plastic guidewire is placed over the metallic guidewire followed by the tapered dilator. The tapered dilators are marked to identify the level of dilation fitting the sized tracheostomy tube to be placed; proceed slowly with continued effort as you are dilating.Ultrasonography prior to the procedure reviews the anatomy and assesses for anomalous vasculature that risks bleeding. It may also be of benefit in confirming the guidewire presence in the tracheal lumen. This is especially helpful if any questions arise during the procedure, so ultrasound should be available at the time of the procedure. This can also be done by bronchoscopy.
Once fully dilated, the TT is inserted over the guidewire left in place once the dilator was removed. Again, maintaining the patient in the fully extended position is key to performing this step smoothly.
Remove the trochanter from the TT, replace it with the inner cannula and connect to the ventilator. Do not extubate unless the patient is receiving full tidal volumes on the ventilator (remember air escaping from the ET may falsely diminish tidal volumes); listening to breath sounds and assessing O2 saturation and end‐tidal CO2 will help verify TT placement.
Remove the ETT, suture the TT in place and order a CXR to rule out PTX.
Bronchoscopic assistance
The use of bronchoscopic guidance during tracheostomy is not routinely required and in at least one study did not result in better outcomes.
It allows for positioning of the ETT and the placement of the needle under direct visualization.
Bronchoscopy may be of more use in complicated cervical collar patients or the obese; or acutely if uncertainties arise during the procedure.
The advantages of bronchoscopy include: real‐time needle‐tip localization during the procedure with less needle punctures; confirmation of endoluminal placement and supracarinal measurement; and if there is dislodgment of the ETT or TT during the procedure it can guide replacement.
The disadvantages include: additional equipment and personnel (bronchoscopist) and greater cost. Bronchoscopy can obstruct the airway with possible impaired ventilation.
Management of complications
Pneumothorax: in the event of deterioration from a diagnosed or suspected PTX, immediately place a needle anteriorly between the first and second ribs, and bilaterally unless unilateral PTX is obvious.
PTX can also present later, which is why a CXR always follows the procedure. If pneumothorax is present, a chest tube is required to prevent the development of tension pneumothorax.
Follow‐up
Standard tracheostomy care and gradual weaning from the ventilator is followed.
De‐cannulation is considered when the patient is breathing spontaneously without mechanical ventilation for a specified period of days, demonstrates reduced secretions, is able to cough secretions through the mouth, and has a patent airway.
Reading list
1 Freeman BD, Morris PE. Tracheostomy practice in adults with acute respiratory failure. Crit Care Med 2012; 40(10):2890–6.
2 Heffner JE. Tracheotomy: application and timing. Clin Chest Med 2003; 24:389–98.
3 Jackson LSM, et al. Percutaneous tracheostomy: to bronch or not to bronch – that is the question. J Trauma 2011; 71:1553–6.
4 Shaw JJ, Santry HP. Who gets early tracheostomy? Evidence of unequal treatment at 185 academic medical centers. Chest 2015; 148(5):1242–50.
5 Yoo DB, et al. Open bedside tracheotomy: impact on patient care and patient safety. Laryngoscope 2011; 121:515–20.
Images
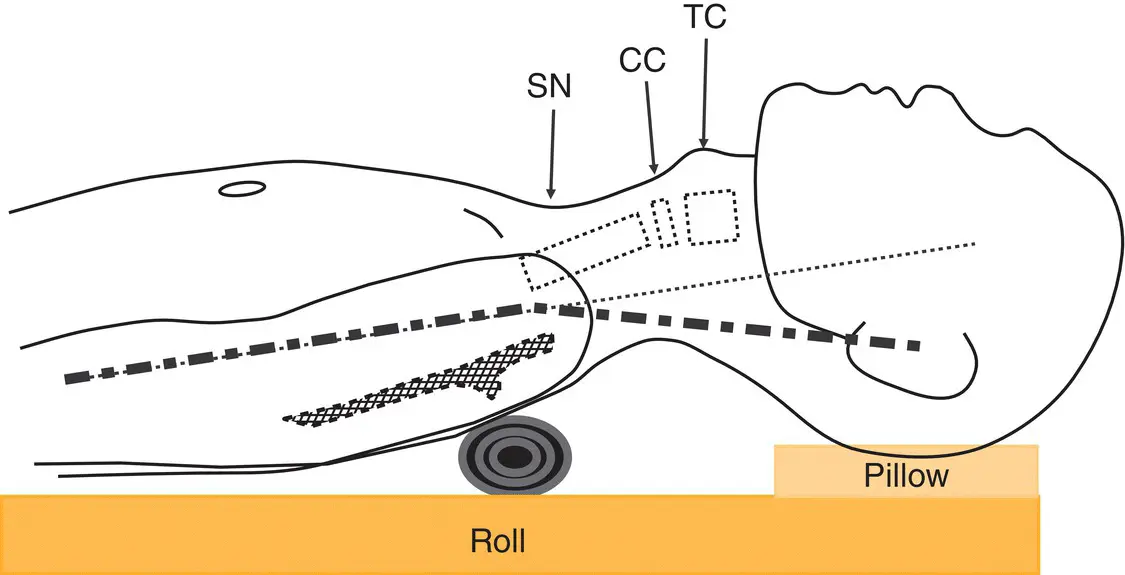
Figure 6.1 Patient positioning for tracheostomy. Place ‘roll’ under shoulder blades to maximize neck extension. Place a pillow under the head until you are ready to start. TC, thyroid cartilege; CC, cricoid cartilage; SN, suprasternal notch.
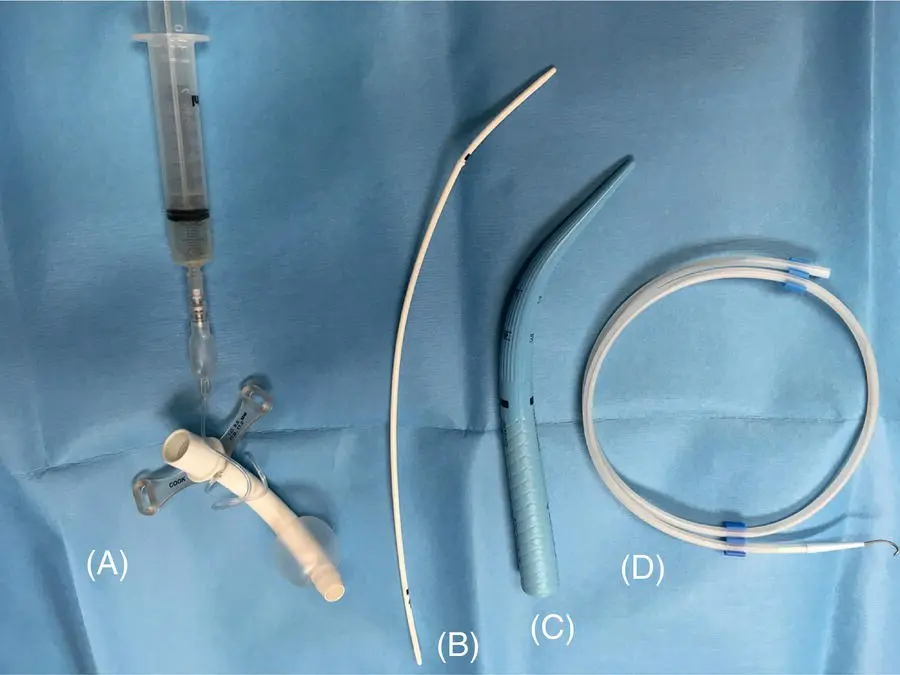
Figure 6.2 The essentials found in most percutaneous tracheostomy kits. (A) Tracheostomy tube with cuff inflated. (B) Plastic guidewire sheath with bulge at the top end to avoid posterior trachea injury from the dilator. (C) Tracheotomy tapered dilator. (D) Guidewire.
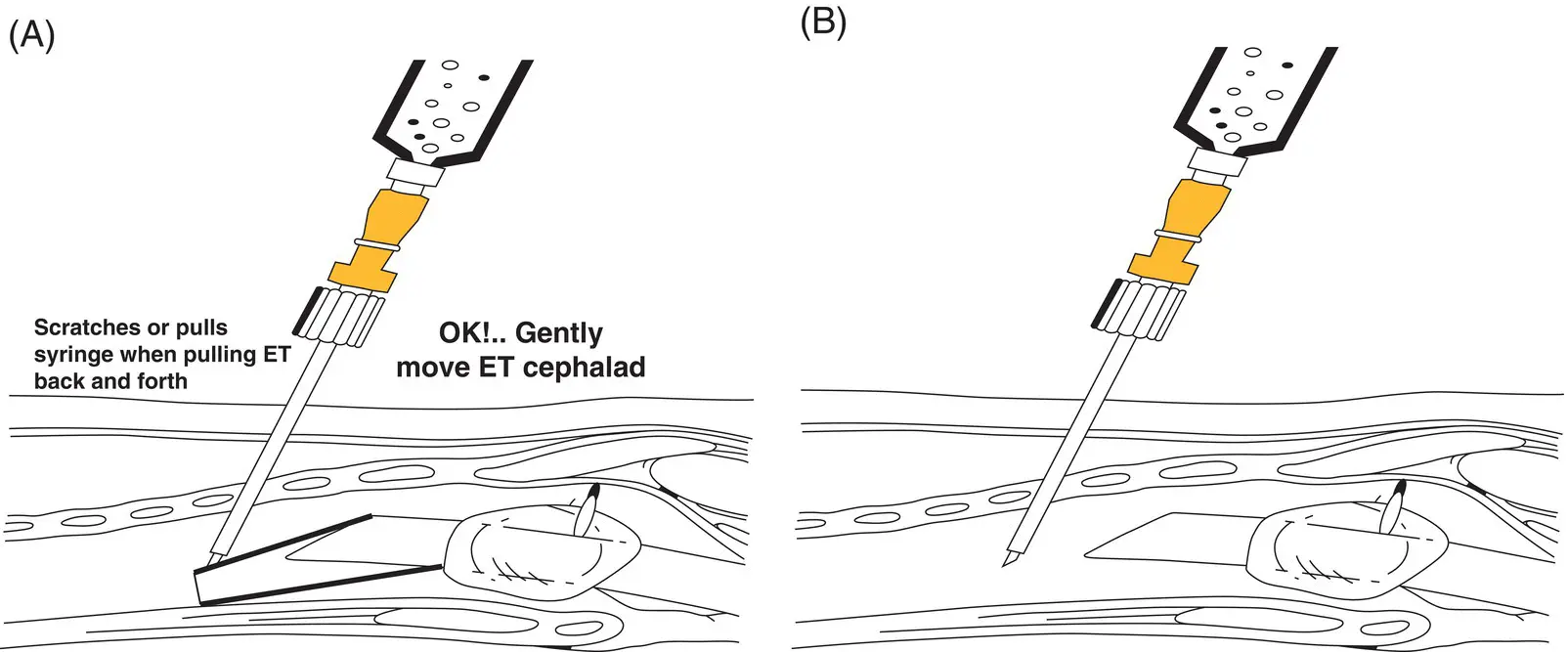
Figure 6.3 How to avoid scraping the ET. (A) Needle scraping the ET. (B) Gently move ET cephalad.
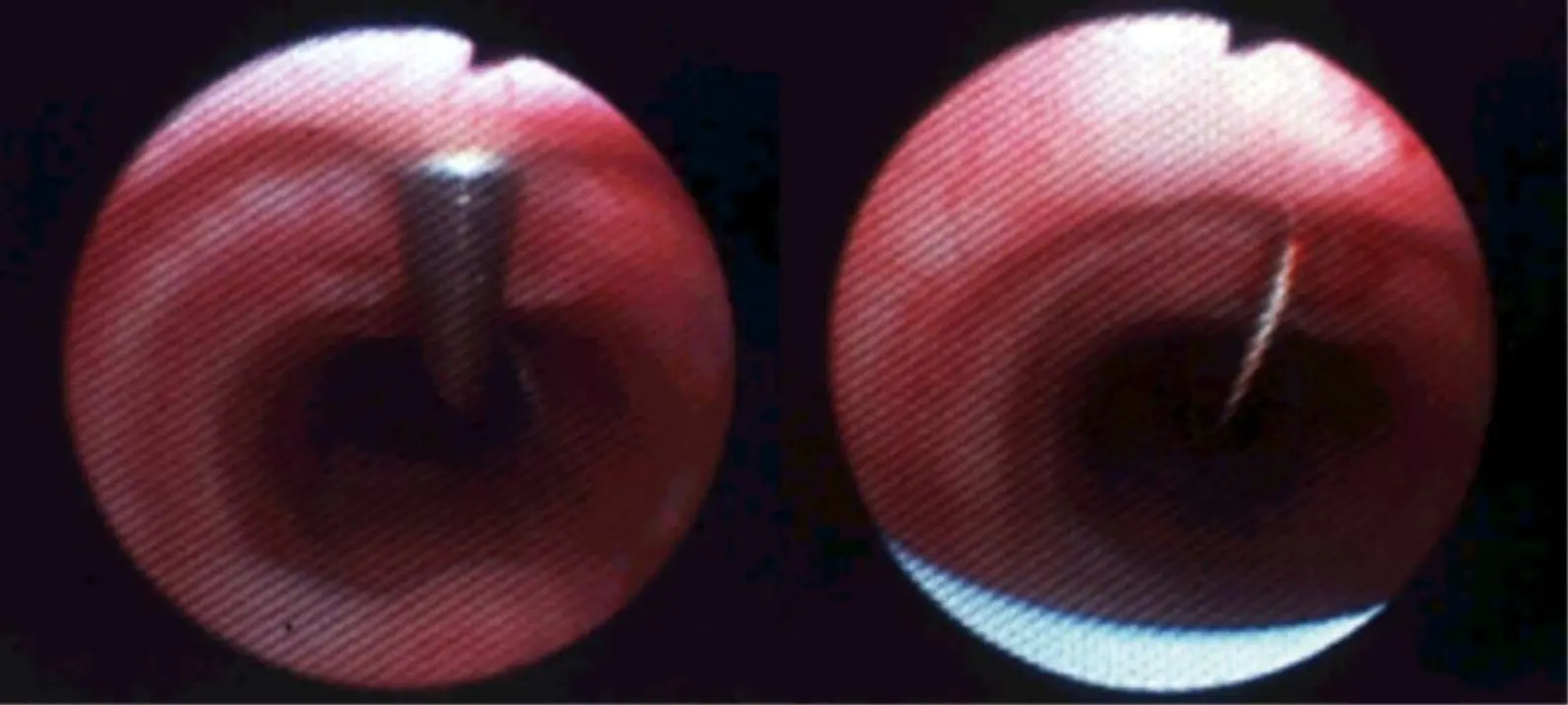
Figure 6.4 Needle and guidewire.
Additional material for this chapter can be found online at:
www.wiley.com/go/mayer/mountsinai/criticalcare
This includes multiple choice questions and Video 6.1. The following image isavailable in color: Figure 6.4 .
CHAPTER 7 Nutritional Support and Total Parenteral Nutrition
Rohit R. Gupta and Roopa Kohli‐Seth
Icahn School of Medicine at Mount Sinai, New York, NY, USA
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Mount Sinai Expert Guides»
Представляем Вашему вниманию похожие книги на «Mount Sinai Expert Guides» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.











Обсуждение, отзывы о книге «Mount Sinai Expert Guides» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.