Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Caudal Vena Cava
The CVC can mimic pleural effusion in haste, especially at the level of the diaphragm (see Figure 6.16).
Stomach Wall
Typically, the sonographer should stay away from the area of the stomach during the DH view by directing the probe far cranially, striving for the proportionality shown (see Figures 6.15and 6.16). The stomach has a sonolucent (dark or black) component to its wall, which typically appears linear in real‐time imaging but can appear as an anechoic triangulation like free fluid. The stomach wall is also subject to artifacts such as edge shadowing (see Figure 3.2). The best way to avoid being confounded by the stomach is to stay further cranially when interrogating the DH view, understanding that little is gained by imaging caudally toward the stomach during an AFAST (see Figure 5.10). Free intraabdominal fluid is most commonly, easily, and accurately seen between liver lobes along the diaphragm, or between the liver and diaphragm (see Figure 6.10).
Pearl:Stay away from the stomach region because it is too far caudal for the DH view. Free fluid is better appreciated between the liver and diaphragm, between liver lobes more cranially along the diaphragm, and the liver and falciform fat.
Minimizing False Negatives
Repeat AFAST serially four hours post admission as standard of care (or sooner as clinical course dictates) and routinely repeat after resuscitation and rehydration (Lisciandro et al. 2009; Lisciandro 2011; Boysen and Lisciandro 2013). The four‐hour postadmission rule of thumb is supported in human medicine by the American College of Emergency Physicians (ACEP) guidelines ( www.acep.org) as standard of care and has been shown to increase FAST sensitivity, improve patient management, and prevent the “crump factor” in people with hypotension (Blackbourne et al. 2004; Ollerton et al. 2006; Bilello et al. 2011). In the AFAST study, ~20% of dogs changed score on serial examination, most worsening with increasing abdominal fluid scores (Lisciandro et al. 2009).
Serial AFAST Examinations Increase Sensitivity
Don’t sweat questionable small pockets of free fluid. Serially repeat AFAST at least one more time four hours later (and sooner if the patient is questionable or unstable). The serial AFAST examination provides another opportunity to screen for free fluid that was absent or questionable that may now be easily seen as present (Lisciandro et al. 2009; Lisciandro 2012; Blackbourne et al. 2004), and to rescore (AFS) for worsening (increasing AFS), static (same AFS), or improving (decreasing AFS) (Lisciandro et al. 2009, 2019). Free fluid also may become safely accessible for sampling in previously lower‐scoring patients, which can be hugely helpful in decision making between medical and surgical cases. Knowing whether a patient is fluid positive helps maximize fluid resuscitation (Ollerton et al. 2006).
AFAST Spleno‐Renal View
| Questions Asked at the SR (HR) View a | |
| Is there any free fluid in the abdominal (peritoneal) cavity? | Yes or no |
| How much free fluid is at the SR view using the AFAST AFS system? | 0, 1/2, 1 |
| What does the left (right when in left lateral) kidney look like? b | Unremarkable or abnormal |
| What does the spleen (liver when in left lateral) look like? b | Unremarkable or abnormal |
| Could I be misinterpreting an artifact or pitfall as pathology? | Know pitfalls and artifacts |
aNote that this view is the SR view in right lateral recumbency and the HR view in left lateral recumbency.
bIt is important to know that the AFAST target‐organ approach for parenchymal abnormalities is binary as “unremarkable” or “abnormal” to capture the case for additional imaging and confirmatory testing. More interpretative skills may be gained through experience, and additional ultrasound study and training.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX,
The SR view includes visualization of both the spleen (peritoneal cavity) and the left kidney (retroperitoneal space) ( Figures 6.17and 6.18).
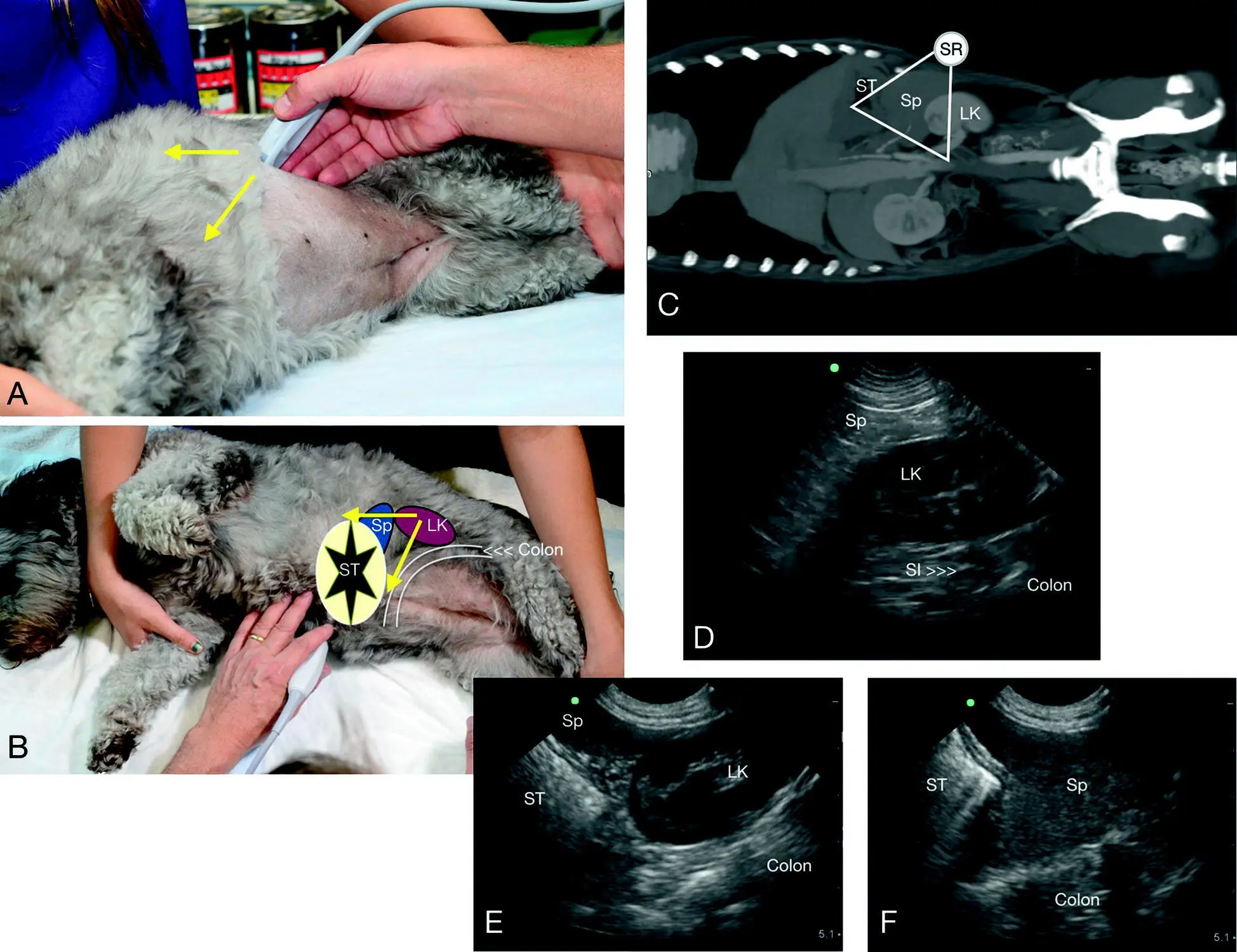
Figure 6.17. The SR view in a dog. In (A) is the external location where the ribs meet the hypaxial muscles dorsally, followed by (B) through (F) showing the relevant anatomy that includes the left kidney, the head of the spleen where it attaches to the greater curvature of the stomach, and the viscus often air‐filled stomach cranially and colon caudally. Ultrasound cannot image past air and thus each organ causes dirty shadowing. The left kidney is retroperitoneal and the spleen is peritoneal. LK, left kidney; SI, small intestine; Sp, spleen; ST, stomach. Computed tomography courtesy of Dr Daniel Rodriguez, VETTEM, and Dr Jesús Paredes, CVM, Mexico City, Mexico.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
The SR target organs are readily imaged in the preferred positioning of right lateral recumbency by placing the probe just caudal to the last rib and dorsally where the rib and the hypaxial muscles meet. The probe is fanned in both directions in longitudinal (sagittal) orientation, recalling that the left kidney is protected by the hypaxial muscles, and in close proximity to the great vessels because of the short renal artery and vein to the aorta and CVC, respectively.
If the left kidney is not located, the probe is rocked cranially under the costal arch and then again fanned since in most dogs the left kidney would tend to be located more cranial than caudal to your starting point.
Once the left kidney is located, it is interrogated by making it as longitudinally symmetrical as possible, and then fanning through it longitudinally (sagittal) in both directions for any free fluid and any obvious renal and perirenal pathology.
The probe is then rocked cranially to search for the head of the spleen, recalling that in dogs and cats, the spleen is reliably found because it is attached by its short gastric vessels to the greater curvature of the stomach in this region.
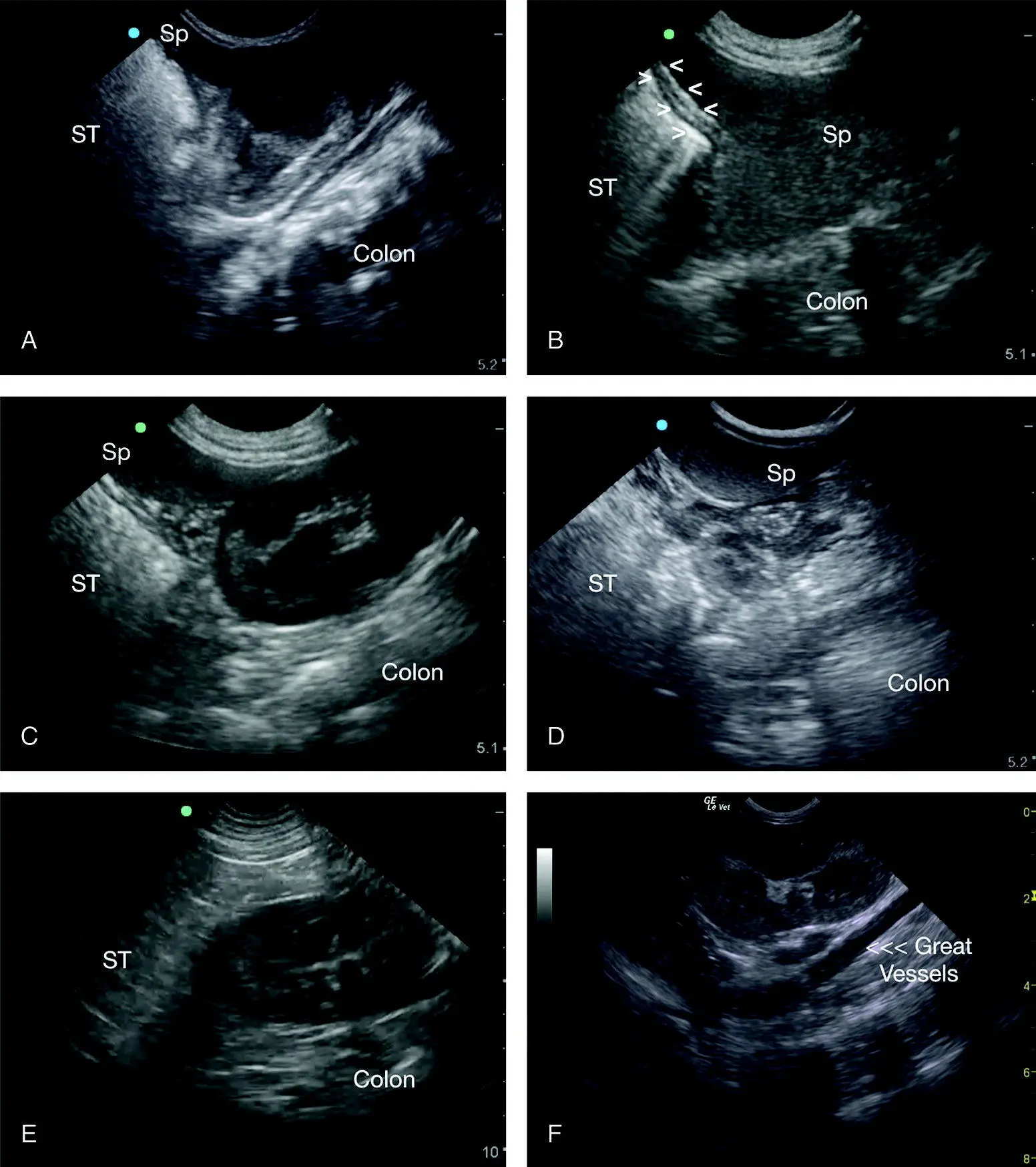
Figure 6.18. Examples of typical negative studies at the SR view. In (A) the air‐filled stomach (ST) and the colon shadow through the far‐field, giving the SR view its characteristic pie‐piece of information with the head of the spleen (Sp) abutting the left kidney. In (B) the wall of the stomach is outlined (V) and a large swath of the head of the spleen is fanned and interrogated while remaining at the SR view's external location. Do not wander from this region to look for the spleen (see Focused Spleen below). In (C) is another example of the target organs of the head of the spleen and the left kidney being in view. In (D) interposing small intestine is past the spleen to the far‐field (“hamburger” look of small intestine) without the left kidney target organ. (E) shows the left kidney without the spleen target organ, which will require rocking the probe cranially. In (F) are the left kidney and adjacent great vessels, keeping in mind the retroperitoneal anatomy includes the CVC, the aorta, renal artery and vein, and adrenal glands. Note the consistency in the images with their proportionality and location of the relevant SR view structures of the left kidney, spleen, stomach, and colon.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.