Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
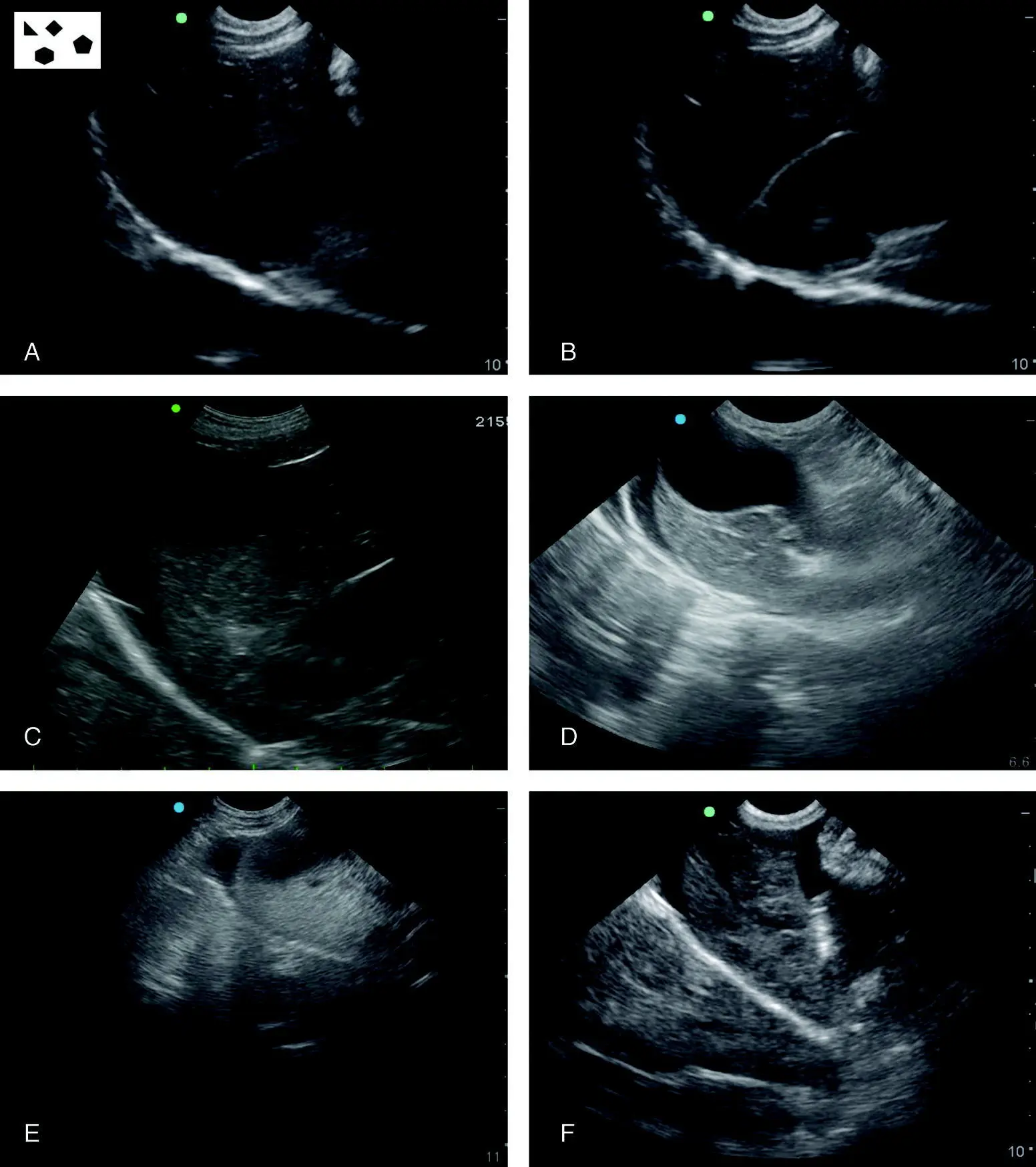
Figure 6.10. Variety of typical positive studies at the DH view. In (A) free fluid is apparent in the near‐field to the gallbladder. In (B) similarly free fluid is in the near‐field to the gallbladder. In (C) free fluid separates the liver from the diaphragm. In (D) there is a smaller abdominal effusion present separating the liver from the diaphragm. In (E) the same type of positive as in (D) is shown but with an even smaller volume. Note the probe is rocked cranial enough to get the diaphragm at the xiphoid, which is good practice for the DH view. In (F) the liver lobes are separated from one another due to the abdominal effusion. Note how consistent the diaphragm is within the images as a landmark for proper DH view image acquisition.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
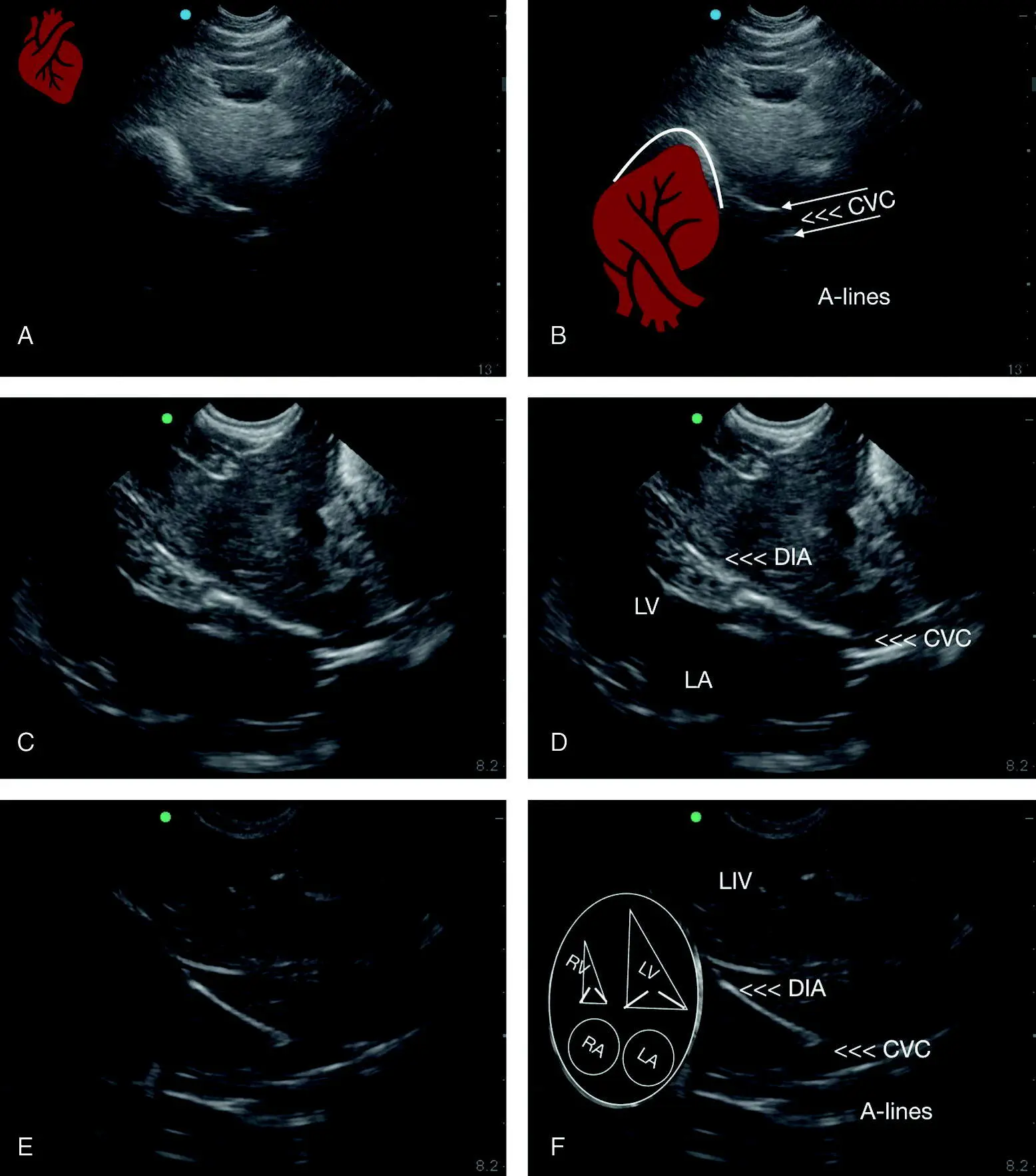
Figure 6.11. The “cardiac bump” at the DH view. In (A) the apex of the heart is indenting the diaphragm and in real time can be seen clearly beating against the diaphragm. In (B) a heart is superimposed to give a better idea of orientation. The arrows point out the near and far wall of the caudal vena cava (CVC). In (C) the heart is unlabeled with the left ventricle and left atrium both in view as well as the mitral valves with the same image labeled in (D) and the heart is positioned similar to the pictorial of the heart in (F). This cardiac orientation is really important to learn because the heart is generally more sonographically accessible than transthoracic TFAST pericardial site views and its echo views in respiratory distressed patients. In (E) is the unlabeled heart against the diaphragm and labeled with the addition of an overlay of the cardiac orientation in (F). Note how consistent the placement of the diaphragm is within the images as a landmark for proper DH view image acquisition. CVC, caudal vena cava; DIA, diaphragm; LA, left atrium; LIV, liver; LV, left ventricle; RA, right atrium; RV, right ventricle.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Following interrogation of the pleural cavity, pericardial sac, and lung along the diaphragmatic–pulmonary interface, along the same longitudinal plane of the “cardiac bump,” look for the CVC, making sure depth is adequate as the CVC is the deepest structure at the DH view ( Figure 6.12).
If the CVC is not seen, look for it while you rock slowly back to your starting point, making sure you are on a longitudinal plane on midline and immediately caudal to the xiphoid.
The CVC is reliably imaged with experience and should be characterized where it traverses the diaphragm, searching for the small white line in the near‐field and the longer white line in the far‐field paralleling one another and representing the near and far walls of the CVC, respectively. The lines that extend beyond the CVC's far wall are in fact A‐lines created when aerated (dry) lung (most common) is immediately against the far wall or possibly in the presence of pneumothorax (far less common) (see Figure 6.12).
Pearl:Excessive probe pressure caused by pushing the probe into the patient's abdomen can distort the CVC, resulting in its flattening and false assessment (Darnis et al. 2018).
Typical DH Positives
The classic intraabdominal positives at the DH view are usually seen while fanning away from the tabletop in the following locations: the near‐field to the gallbladder, between the divisions of the liver lobes, between the liver and the diaphragm, and between the liver lobes and the falciform ligament and fat. In the near‐field, the falciform ligament and fat, which can be robust even in thin cats, are typically hyperechoic (bright) in the near‐field, having a coarser, brighter echotexture (hyperechoic) relative to the liver (see Figure 6.10and Chapter 39).
The most common AFAST positive views in low‐scoring AFS 1 and AFS 2 bluntly traumatized dogs and cats, clinically normal adult dogs and cats, and juvenile puppies and kittens are the nongravity‐dependent DH and CC views over the most gravity‐dependent HRU and SRU views (Lisciandro et al. 2009, 2015, 2019). Moreover, the umbilical HRU and SRU views are rarely the only positive view(s) among different subsets of dogs and cats (Lisciandro et al. 2009, 2015, 2019; Romero et al. 2015). Thus, pay special attention to the presence of anechoic triangles (free fluid) while fanning through liver lobes (see Figure 6.10).
Artifacts and Pitfalls of the DH View
The DH View has many, if not all, the described ultrasound artifacts, including mirror image, acoustic enhancement, edge shadowing, side‐lobe and slice‐thickness (see Chapters 3and 5). It is very important to be familiar with these common artifacts at the DH view ( Figure 6.13). These same artifacts are possible at the CC view (see Figure 6.26), another AFAST view with a fluid‐filled structure (DH view – gallbladder, CC view – urinary bladder).
Pearl:A good learning exercise is to focus on a specific artifact and then look through several DH view video clips from different patients looking for that specific artifact.
Artifacts
Mirror Image Artifact
The DH view is the classic example for mirror image artifact, which requires a strong air–soft tissue interface such as between the lung diaphragm and liver (see Figure 6.13). As a result, the ultrasound machine's software displays the liver and its structures as mirrored into the thoracic cavity (see Chapters 3and 5).
Common DH view mirror image artifact misinterpretations include the following.
The liver and gallbladder mirrored into the thorax and mistaken for a diaphragmatic hernia.
The gallbladder mirrored into the thorax and mistaken for pleural and pericardial effusion, noting that a “partial” mirroring of the gallbladder can occur.
Ascites mirrored into the thorax can be mistaken for pleural and pericardial effusion, and liver appearing as lung, noting that a “partial” mirroring of ascites can occur.
Acoustic Enhancement Artifact
The gallbladder will make the soft tissues distal to its fluid‐filled luminal contents appear much brighter (more echogenic or hyperechoic) than adjacent soft tissues, similar to what occurs with the fluid‐filled urinary bladder (see Figure 6.26). Typically, the acoustic enhancement includes a brighter liver and sometimes B‐lines through the far‐field to the fluid‐filled gallbladder ( Figure 6.14) (see Chapters 3and 5); however, when lung is truly dry, no B‐lines should be seen through the acoustic enhancement, unless the lung is truly “becoming” wet (see Chapters 22and 23).
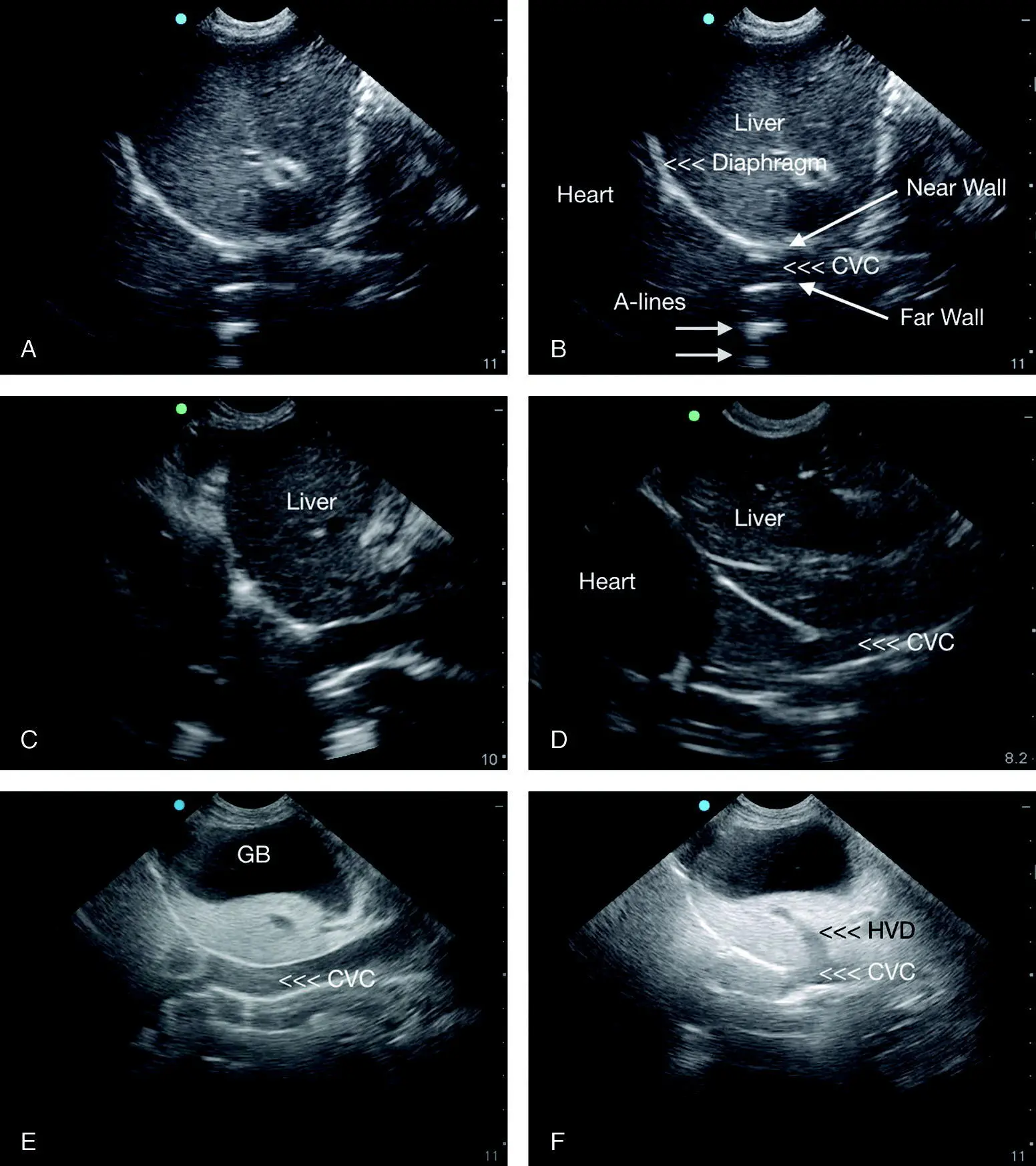
Figure 6.12. Variety of typical CVC images with other relevant structures. (A) Unlabeled DH view with the CVC followed by (B) labeled view of the same image. In (C) the CVC is obvious with its near and far wall and its maximum diameter, which may be eyeballed for its approximate measurement from the centimeter scale to the right of the screen. In (D) structures are labeled and similarly positioned as in (C). In (E) the CVC is distended and conspicuous due to right‐sided heart failure. In (F) the DH view is fanned slightly from where in (E) the hepatic venous distension, referred to as the “tree trunk sign” (Lisciandro 2014a, 2016a), is apparent (see also Figure 36.8). Note how consistent the diaphragm is within the images as a landmark for proper DH view image acquisition. CVC, caudal vena cava; GB, gallbladder; HVD, hepatic venous distension.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.