Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood. TX. Illustration by Hannah M. Cole, Adkins, TX.
Modified Lateral‐Sternal
Modified lateral‐sternal recumbency positioning may be used for AFAST in stressed patients by allowing the forelegs to be in sternal and moving the hindlegs together laterally (placed same side as the sonographer) ( Figure 6.4). In the modified lateral‐sternal positioning the AFS may be estimated because the patient isn't purely in a lateral recumbent position.
Standing/Sternal
In respiratory‐compromised patients AFAST is performed in standing or sternal knowing that the fluid scoring system is not validated in this positioning but still provides clinical information regarding the presence or absence of effusion. Whatever the AFAST options for positioning (lateral, modified lateral‐sternal, standing/sternal), a negative AFS negates the need for moving the patient to lateral recumbency. Serial exams are always mandated as standard of care for a second opportunity to detect negative AFAST changing to positive, and for rescoring the patient (Lisciandro et al. 2009; Lisciandro 2011, 2014a; Boysen and Lisciandro 2013). See Chapters 36and 37for the most efficient ways to perform AFAST in standing‐sternal positioning.
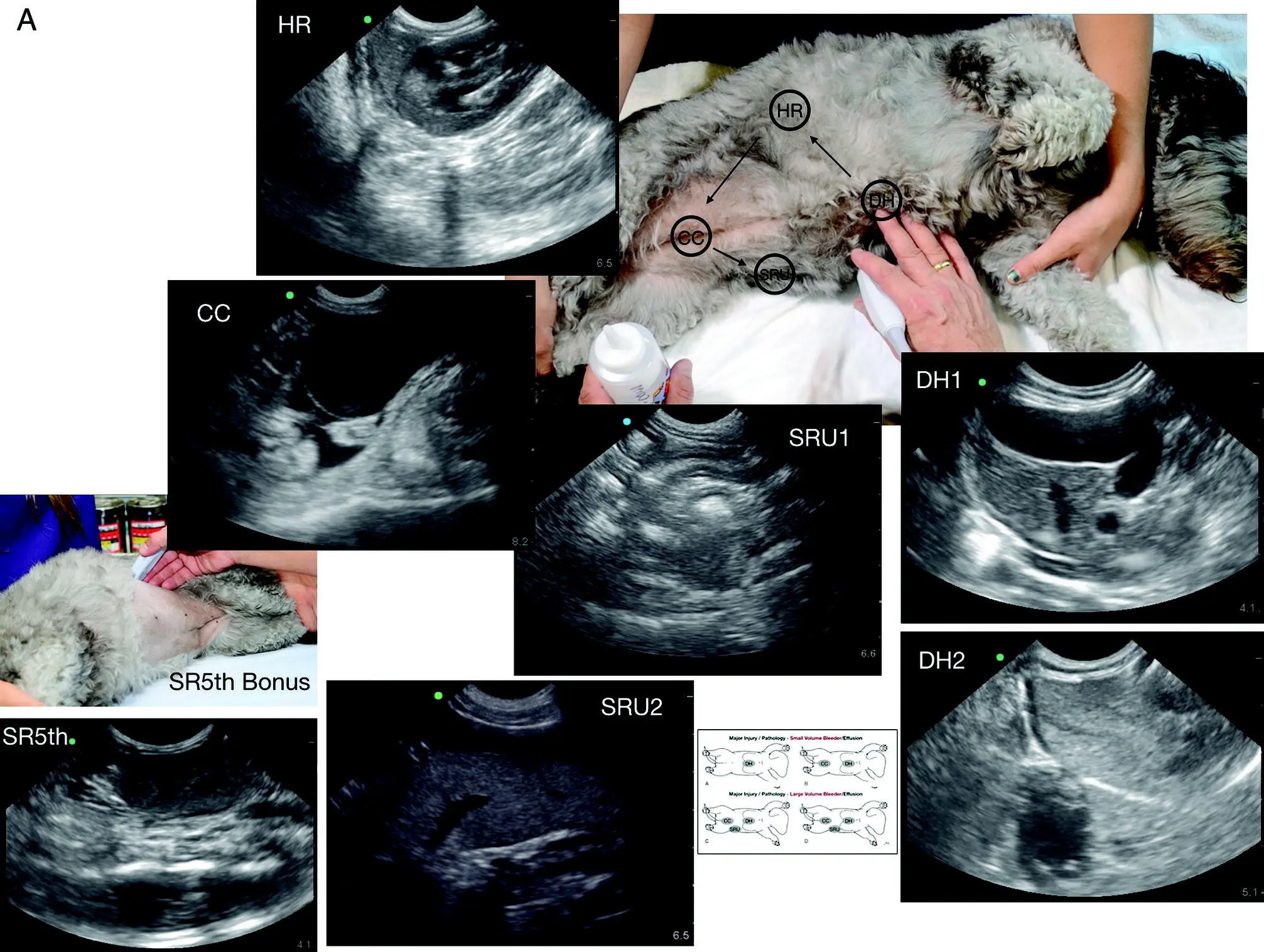
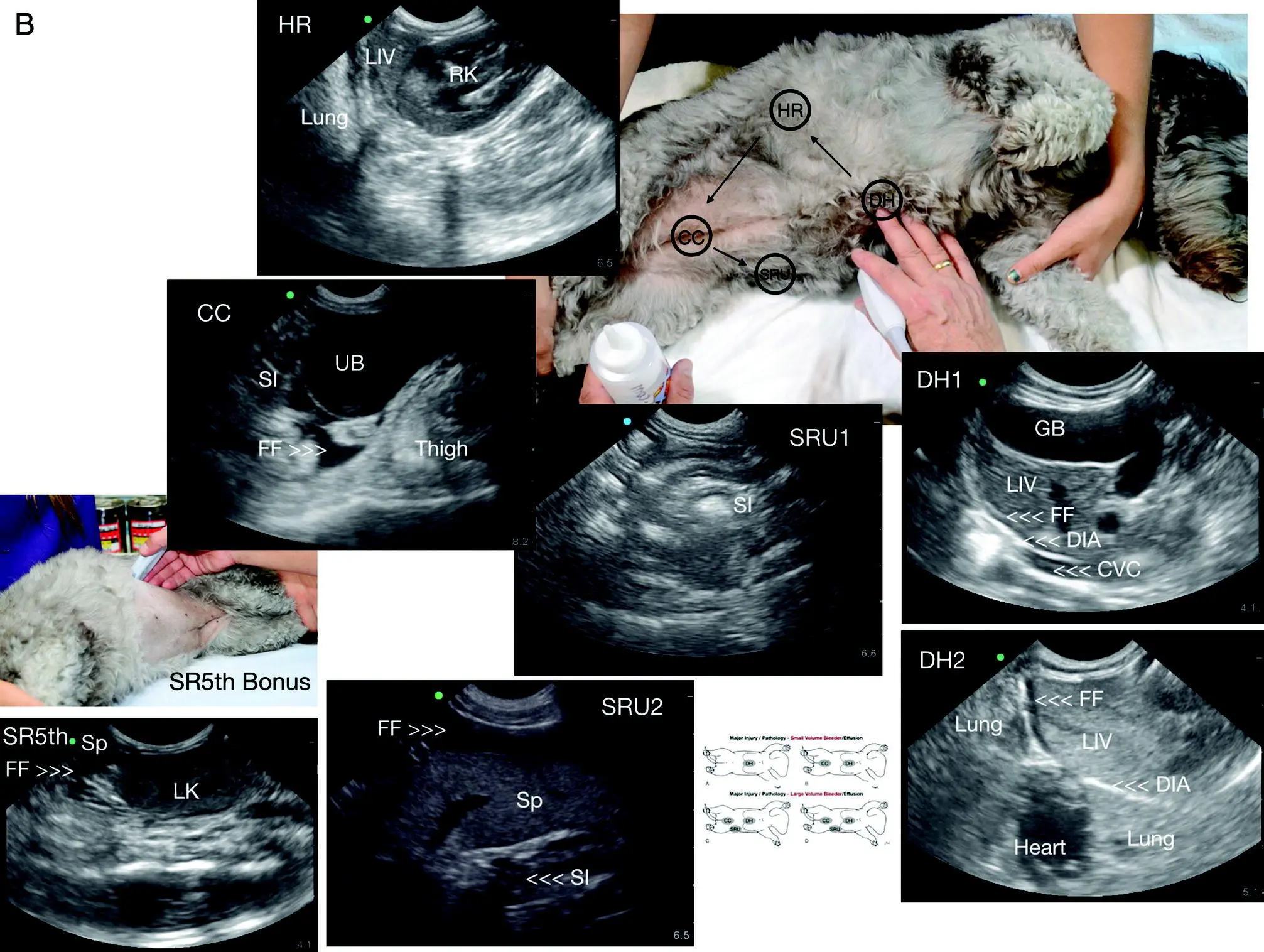
Figure 6.3. AFAST and its five views performed in left lateral recumbency in a dog. Shown is AFAST unlabeled in left lateral recumbency with the same images as Figure 6.2A and B. The order is analogous and always the same as follows: DH to HR to CC to SRU to SR5th bonus view. The final SR5th bonus view is not part of the abdominal fluid score. DH, diaphragmatico‐hepatic view; DH1, DH 1 of 2 views; DH2, DH 2 of 2 views; SR, spleno‐renal view; CC, cysto‐colic view; HRU, hepato‐renal umbilical view; HR5th, hepato‐renal 5th bonus view; HRU1, 1 of 2 views; HRU2, 2 of 2 views. DIA, diaphragm; FF, free fluid; GB, gallbladder; LIV, liver; LK, left kidney; RK, right kidney; SI, small intestine. Note that the images should look identical for each AFAST view regardless of positioning (including standing/sternal, modified sternal). AFAST views are nearly identical no matter the positioning because the respective target organs are imaged with the same methodology.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX. Illustration by Hannah M. Cole, Adkins, TX.
Considerations When Performing AFAST in Standing or Sternal Positioning
If AFAST is negative in standing or sternal positioning, then moving the patient to lateral recumbency is unnecessary. However, if the AFAST examination is positive in standing or sternal, then move the patient to lateral recumbency (if unstable, delay until more stable) and wait for three minutes for fluid to settle before assigning an AFS (Lisciandro et al. 2009; Lisciandro 2011; Boysen and Lisciandro 2013).
When performing AFAST in standing or sternal, the sonographer must keep in mind the following points.
As long as the AFAST is negative and the target organs are imaged at each respective view, the AFAST is complete.
When free intraabdominal fluid is present, it will pool in different regions relative to the target organs because gravity‐dependent locations differ from lateral recumbency, being at the probe head, in the near‐field, for the DH, CC, and SR/HR umbilical views.
The gravity‐dependent regions within the lumen of the gallbladder and urinary bladder also differ from lateral recumbency and the sonographer must consider the direction of the beam (its scanning plane) to best detect and interpret findings.
The AFAST views, when performed properly, should look nearly the same independent of positioning.
Dorsal recumbency should never be used for AFAST (TFAST and Vet BLUE) for several reasons but most importantly because of increasing patient risk ( Figure 6.5). A hemodynamically fragile patient placed in dorsal recumbency undergoes significant negative changes in ventilation and circulation, specifically venous return. Add to these respiratory and cardiovascular stresses and the increased oxygen demand in a struggling, anxious patient, and the patient risks acute and potentially catastrophic decompensation. Considering trauma, most dogs and cats have concurrent lung contusions and other thoracic‐related injuries (Powell et al. 1999; Sigrist et al. 2011; Lisciandro et al. 2008) and intraabdominal bleeding (Boysen et al. 2004; Lisciandro et al. 2009). Considering nontrauma, many hypotensive triaged patients have pleural and/or pericardial effusion, and intracavitary bleeds often accompanied by anemia (McMurray et al. 2016; Lisciandro 2016a,b). Moreover, the AFS system is not validated in dorsal recumbency and only subjective terms of mild, moderate, and severe can be used (Stander et al. 2010; Sutherland‐Smith et al. 2006). For clinicians who prefer performing complete detailed abdominal ultrasound in dorsal recumbency, perform a Global FAST first before moving the patient to the restraint of dorsal recumbency to best ensure patient safety.

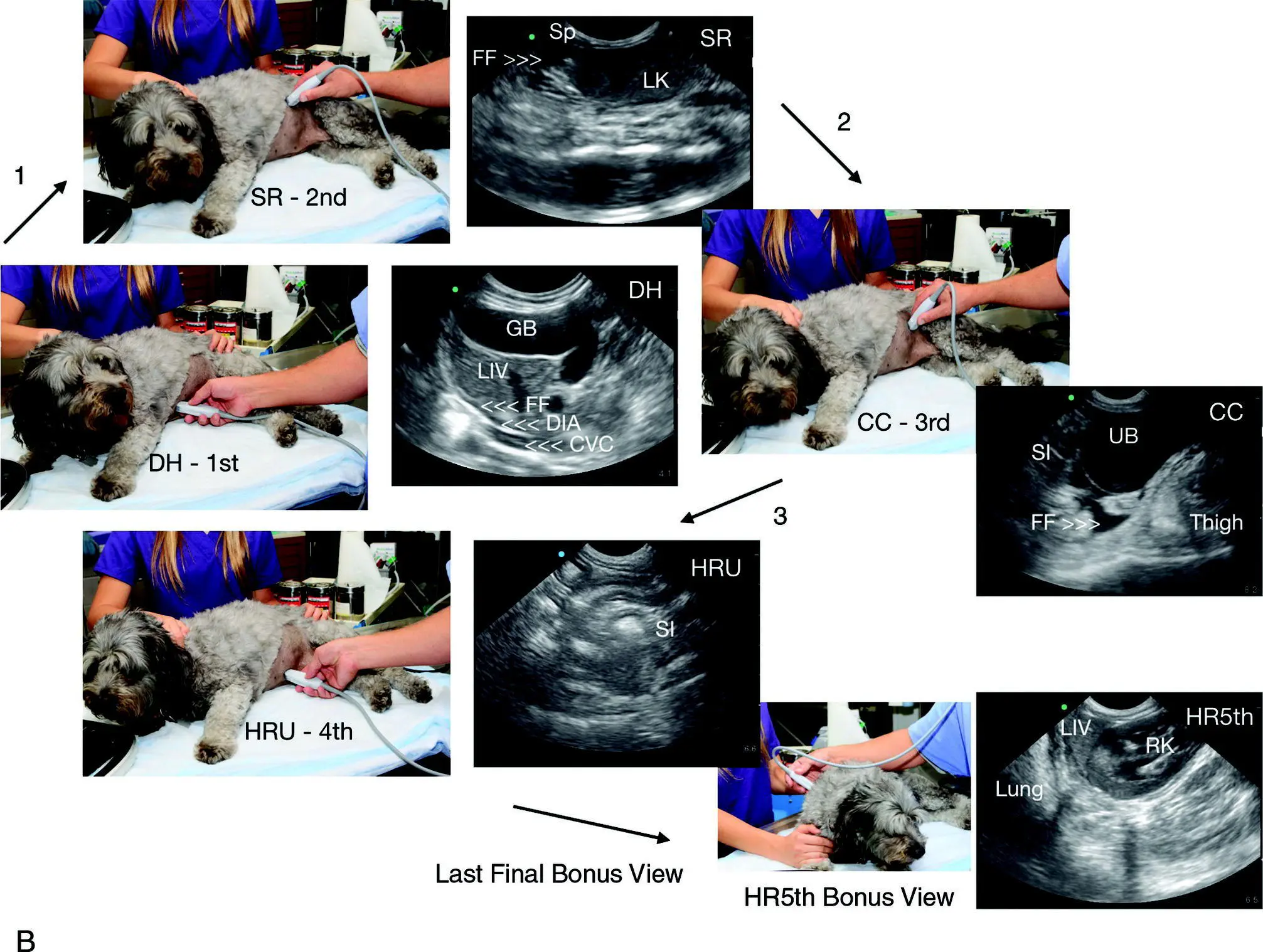
Figure 6.4. Modified lateral‐sternal recumbency. The AFAST views are performed in the same order every time as follows: DH to SR to CC to HRU to HR5th bonus view. The final HR5th bonus view is not part of the abdominal fluid score.DH, diaphragmatico‐hepatic view; SR, spleno‐renal view; CC, cysto‐colic view; HRU, hepato‐renal umbilical view; HR5th, hepato‐renal 5th bonus view. Note that the images should look identical for each AFAST view regardless of positioning (including standing/sternal, modified sternal). AFAST views are nearly identical no matter the positioning because the respective target organs are imaged with the same methodology.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Naming and Order of the AFAST Views
The AFAST sites in the preferred positioning of right lateral recumbency (over left) are named according to target organs at each acoustic window and performed in clockwise order as follows: (1) DH view, (2) SR view, (3) CC view, and (4) HR umbilical (HRU) view that completes the AFAST examination and is a favorable site for abdominocentesis, being most gravity dependent (Lisciandro et al. 2009; Lisciandro 2011; Boysen and Lisciandro 2013; McMurray et al. 2016). AFAST views are shown translated onto an abdominal radiograph and CT study in Figure 6.6. The final view is the HR5th bonus view to image the right kidney and nearby liver that is not part of the AFS; the HR5th bonus view is generally performed as the final view after AFAST, TFAST, and Vet BLUE have been completed.
In LL recumbency the order is as follows: (1) DH view, (2) HR view, (3) CC view, and (4) the SR umbilical (SRU) view that completes the AFAST examination and is a favorable site for abdominocentesis, being most gravity dependent (see Figure 6.3). Positioning of the cat is shown in Chapter 39. The final view is the SR5th bonus view to image the left kidney and spleen and is not part of the AFS; the SR5th bonus view is generally performed as the final view after AFAST, TFAST, and Vet BLUE have been completed (Lisciandro et al. 2009; Lisciandro 2011; Boysen and Lisciandro 2013; McMurray et al. 2016).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.