James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The location of the stress-breaking device in the five-unit pier-abutment restoration is important. It is usually placed on the middle abutment because placement on either of the terminal abutments could result in the pontic acting as a lever arm.
The keyway of the connector should be placed within the normal distal contours of the pier abutment, and the key should be placed on the mesial side of the distal pontic. The long axes of the posterior teeth usually lean slightly in a mesial direction, and vertically applied occlusal forces produce further movement in this direction. Nearly 98% of posterior teeth tilt mesially when subjected to occlusal forces. 24If the keyway of the connector is placed on the distal side of the pier abutment, mesial movement seats the key into the keyway more solidly 19( Fig 7-24). Placement of the keyway on the mesial side, however, causes the key to be unseated during mesial movements 20( Fig 7-25). In time, this could produce a pathologic mobility in the canine or failure of the canine retainer.
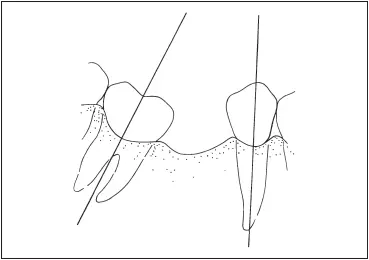
Fig 7-26When a mandibular molar tilts mesially, there is a discrepancy between its long axis and that of the premolar.
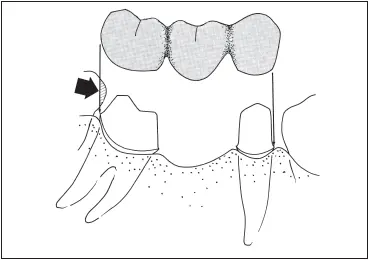
Fig 7-27This fixed partial denture will not seat because the tooth distal to the fixed partial denture intrudes on the path of insertion ( arrow ).
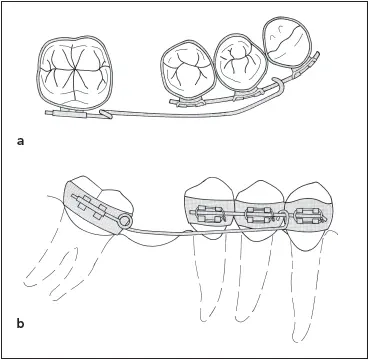
Fig 7-28Orthodontic appliance for uprighting a tilted molar: ( a ) occlusal view; ( b ) facial view.
Tilted molar abutments
A problem that occurs with some frequency is a mandibular second molar abutment that has tilted mesially into the space formerly occupied by the first molar. It is impossible to prepare the abutment teeth for a fixed partial denture along the long axes of the respective teeth and achieve a common path of insertion ( Fig 7-26).
There is further complication if the third molar is present. It usually will have drifted and tilted with the second molar. Because the path of insertion for the fixed partial denture will be dictated by the smaller premolar abutment, it is probable that the path of insertion will be nearly parallel to the former long axis of the molar abutment before it tilted mesially. As a result, the mesial surface of the tipped third molar will encroach upon the path of insertion of the fixed partial denture, thereby preventing it from seating completely ( Fig 7-27).
If the encroachment is slight, the problem can be remedied by restoring or recontouring the mesial surface of the third molar. However, the overtapered second molar preparation must have its retention bolstered by the addition of facial and lingual grooves. If the tilting is severe, more extensive corrective measures are called for. The treatment of choice is the uprighting of the molar by orthodontic treatment. In addition to placing the abutment tooth in a better position for preparation and for distribution of forces under occlusal loading, uprighting the molar also helps to eliminate bony defects along the mesial surface of the root.
Uprighting is best accomplished through the use of a fixed appliance. 25Both premolars and the canine are banded and tied to a passive stabilizing wire ( Fig 7-28). A helical uprighting spring is inserted into a tube on the banded molar and activated by hooking it over the wire on the anterior segment. 25,26This is frequently followed by the use of an open coil spring to complete the uprighting and bring the tooth into the best possible alignment for fabrication of the fixed restoration. The average treatment time required is 3 months. 27
The third molar, if present, is often removed to facilitate the distal movement of the second molar. The second molar will arc occlusally as it moves distally; therefore, it must be watched closely and ground out of occlusion to allow it to continue moving. Immediately upon removal of the appliance, the teeth are prepared, and a provisional fixed partial denture is fabricated to prevent posttreatment relapse. 28
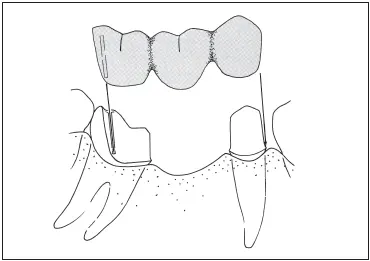
Fig 7-29Fixed partial denture using a proximal half crown as a retainer on a tilted molar abutment.
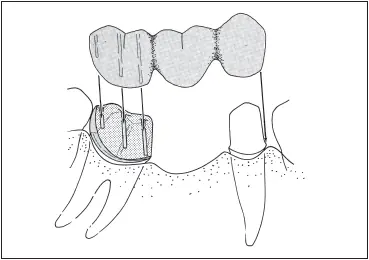
Fig 7-30Fixed partial denture using a telescope crown and coping as a retainer on a tilted molar abutment.
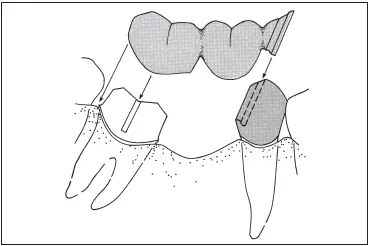
Fig 7-31A nonrigid connector on the distal aspect of the premolar retainer compensates for the inclination of the tilted molar.
If orthodontic correction is not possible, or if it is possible to achieve only a partial correction, a fixed partial denture can still be made. It has been suggested that the long axis of the prospective abutments should converge by no more than 25 to 30 degrees. 29Photoelastic 30and finite element 31stress analyses have shown that a molar that has tipped mesially will actually exhibit less stress in the alveolar bone, along the mesial surface of its mesial root, with a fixed partial denture than without it. There will be an increase in stress along the premolar, however.
A proximal half crown sometimes can be used as a retainer on the distal abutment 32( Fig 7-29). This preparation design is simply a three-quarter crown that has been rotated 90 degrees so that the distal surface is uncovered. This retainer can be used only if the distal surface itself is untouched by caries or decalcification and if there is a very low incidence of proximal caries throughout the mouth. The patient must also demonstrate an ability to keep the area exceptionally clean. If there is a severe marginal ridge height discrepancy between the distal of the second molar and the mesial of the third molar as a result of tipping, the proximal half crown is contraindicated.
A telescope crown and coping can also be used as a retainer on the distal abutment. 33A full crown preparation with heavy reduction is made to follow the long axis of the tilted molar. An inner coping is made to fit the tooth preparation, and the proximal half crown that will serve as the retainer for the fixed partial denture is fitted over the coping ( Fig 7-30). This restoration allows for total coverage of the clinical crown while compensating for the discrepancy between the paths of insertion of the abutments. The marginal adaptation for this restoration is provided by the coping.
The nonrigid connector is another solution to the problem of the tilted fixed partial denture abutment ( Fig 7-31). A full crown preparation is done on the molar, with its path of insertion parallel with the long axis of that tilted tooth. A box form is placed in the distal surface of the premolar to accommodate a keyway in the distal of the premolar crown. It is tempting to place the connector on the mesial aspect of the tipped molar, but this could lead to even greater tipping of the tooth. A nonrigid connector for the tipped molar abutment is most useful when the molar exhibits a marked lingual as well as mesial inclination. Preparing a tooth with a combined mesial and lingual inclination as an abutment for a routine fixed partial denture can lead to a drastically over-tapered preparation with no retention.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.