James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
8 Fixed Partial Denture and Implant Configurations
The replacement of missing teeth with fixed restorations has changed considerably in the last 20 years. No longer is it simply a choice between a fixed partial denture and a removable partial denture. Osseointegrated dental implants have developed into a reliable treatment modality that can be depended upon to provide long-term replacement of a single missing tooth as well as multiple missing teeth. By no means, though, should the fixed partial denture be regarded as a thing of the past. Not all patients or situations are suitable for implants, just as not all patients or situations are suitable for fixed partial dentures. Judicious treatment planning is still of critical importance.
The implant is ideally suited for the replacement of a single tooth if the teeth that would have served as abutments are untouched by caries or previous restorations. On the other hand, if those teeth need extensive restorations, the patient can be saved expense and additional treatment if the restorations also serve as retainers for a fixed partial denture. Long-span prostheses that will place greater demands on the skills of the dentist, on the resistance of the retainers, and on the abutments and their periodontal support can be avoided by using implant-supported fixed partial dentures instead of tooth-supported fixed partial dentures.
The maximum number of posterior teeth that can be safely replaced with a fixed partial denture is usually two. In rare circumstances, three can be replaced, but that should be attempted only under ideal conditions. An edentulous space created by the loss of four adjacent teeth, other than four incisors, is best restored with implant-supported crowns or a removable partial denture. If more than one edentulous space exists in the same arch, even though each could be individually restored with a fixed partial denture or implants, finances may dictate the use of a removable partial denture. This is especially true when the spaces are bilateral and each involves two or more teeth.
Third molars are not shown in any of the examples in this chapter, and no situation is shown in which a third molar would be a prospective abutment. Rarely can third molars be used as abutments because they have been removed from the mouths of so many patients. Even when they are present, they frequently display incomplete eruption; short, fused roots; and/or a marked mesial inclination in the absence of a second molar.
A third molar should be considered as a potential abutment only if it is upright and completely erupted, with little or no mesial inclination and with long, distinctly separate roots. It also must have a healthy cuff of attached, keratinized gingiva that completely surrounds the tooth. The unattached mucosal tissue that frequently surrounds the distal 30% to 60% of third molars will become inflamed adjacent to even a well-fitting crown margin, and the abutment is likely to fail periodontally.
The following examples are given as a reference that applies under ideal conditions, listing the abutment teeth that normally would be used. Retainer designs should be based on adequate retention, esthetics, and conservation of tooth structure. Clinical situations vary widely, and less conservative designs are required when caries, decalcification, or morphologic traits (such as short clinical crowns) dictate. The configurations in the following scenarios assume that the prospective abutments are still in their original positions. If the abutments have drifted, the situation could become less, and on occasion more, demanding, depending on the current position of the tooth. Fewer or additional abutments may become necessary if there has been drifting or bone loss. The ratios shown for root surface areas are intended as a general guideline, based on average tooth dimensions 1,2and root surface areas. 3An abutment-pontic root ratio of 1.0 or greater is considered to be favorable. 4
Conventional partial coverage retainers could be used for many of the prostheses described. However, the reluctance of many patients to accept any display of metal and the lack of dentist familiarity with these preparations require that this design be used only on selected posterior abutments. Likewise, while resin-bonded fixed partial dentures (ie, Maryland bridges) can provide a suitable replacement for single missing teeth, experience with this type of retainer has shown that it demands a well-defined, albeit a very conservative preparation. They are not the “quick and dirty” restorations that some people thought when they first appeared on the scene in the 1980s. They may be used as an intermediate retainer on young patients with teeth that are not fully formed or fully erupted or whose bone is not developmentally stable.
A fixed partial denture can be classified as either simple or complex, depending on the number of teeth to be replaced and the position of the edentulous space in the arch. The classic simple fixed partial denture is one that replaces a single tooth. Dental implants have expanded the treatment possibilities for the replacement of missing teeth markedly. Two scenarios are presented for each missing tooth, describing the use of a conventional tooth-borne fixed partial denture and an implant-supported crown. There are some situations in which a fixed partial denture cannot be placed with a reasonable expectation of success.
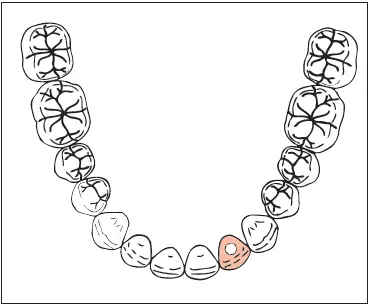
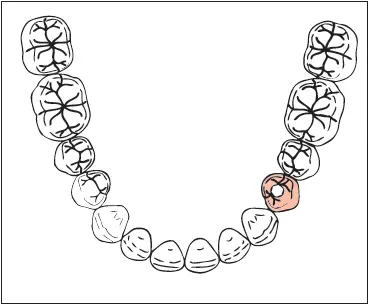
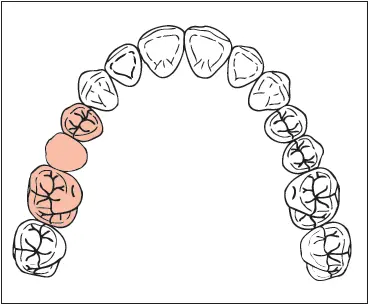
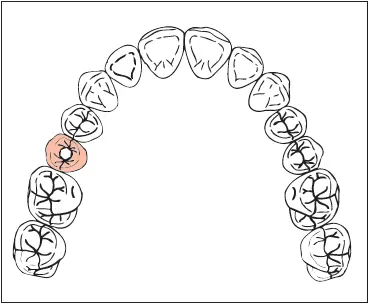
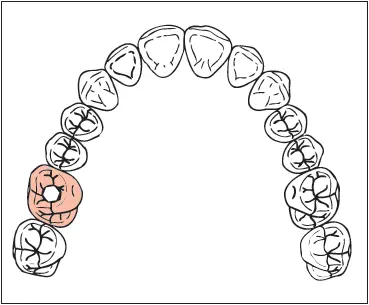
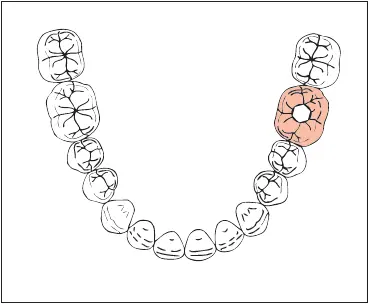
In the scenarios that appear on the following pages, the fixed partial denture solution is followed by the implant solution. In the illustrations, implant restorations are indicated by a shaded tooth with a circle in the center; tooth-borne fixed partial denture retainers are represented by a shaded tooth with contours; and fixed partial denture pontics are shown as a shaded outline of the tooth with no morphology.
Simple Fixed Partial Dentures (One Tooth)
See Table
Complex Fixed Partial Dentures (One Tooth)
See Table
Simple Fixed Partial Dentures (Two Teeth)
See Table
Complex Fixed Partial Dentures (Two Teeth)
See Table
Complex Fixed Partial Dentures (More Than Two Teeth)
See Table
Complex Fixed Partial Dentures (Pier Abutment)
See Table
References
1. Shillingburg HT Jr, Kaplan MJ, Grace CS. Tooth dimensions—A comparative study. J South Calif Dent Assoc 1972;40:830–839.
2. Shillingburg HT, Kessler JC, Wilson EL. Root dimensions and dowel size. CDA J 1982;10:43–49.
3. Jepsen A. Root surface measurement and a method for x-ray determination of root surface area. Acta Odontol Scand 1963;21:35–46.
4. Ante IH. The fundamental principles of abutments. Mich State Dent Soc Bull 1926;8:14–23.
Simple Fixed Partial Dentures (One Tooth)
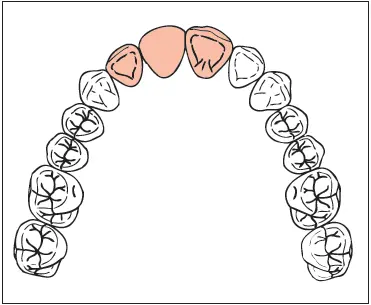 |
Missing: Maxillary central incisor Abutments: Central incisor and lateral incisor Considerations: Abutment discoloration or rotation, improper width of edentulous space, or proximal caries will require metal-ceramic restorations (MCRs). In that eventuality, the crowns can double as retainers, and the space can be restored with a fixed partial denture. Retainers: MCR crowns. Resin-bonded retainers might be used if the patient is very young and if the abutments are healthy teeth that have never been restored. Pontic: Modified ridge lap MCR Abutment-pontic root ratio: 1.9 |
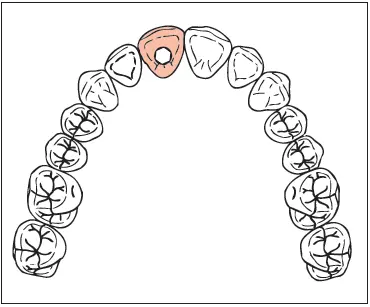 |
Missing: Maxillary central incisor Implant: 4.0 × 12 mm Considerations: A large nasopalatine foramen (incisive canal) may interfere with implant placement. Loss of the facial bone plate may necessitate bone grafting. Restoration: MCR over a custom abutment (UCLA, Atlantis [Astra Tech], or preparable abutment) |
| Missing: Mandibular central incisor Abutments: Central incisor and lateral incisor Considerations: If at all possible, an implant should be used to support this restoration if there is 7.3 mm between the prospective abutments. If there is not, a fixed partial denture will be required. Severely rotated, malposed, or mobile abutments will contraindicate the use of resin-bonded retainers and might dictate the removal of all of the mandibular incisors. In that instance, implants would be placed in the positions of the lateral incisors. If MCR retainers are required for a tooth-borne fixed partial denture, the preparations very easily could encroach on the pulp, and the patient should be so advised. Endodontic treatment and a dowel core would then be necessary. Retainers: Resin-bonded retainers Pontic: Ovate or modified ridge lap MCR (depending on ridge configuration) Abutment-pontic root ratio: 2.1 | 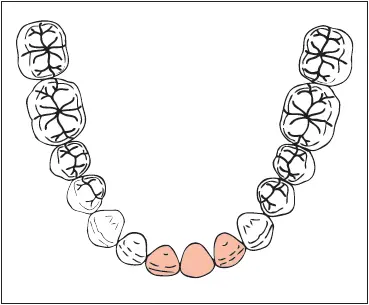 |
| Missing: Mandibular central incisor Implant: 3.3 × 12 mm Considerations: A dental implant is the restoration of choice. The factor limiting replacement of a mandibular central incisor with a dental implant is the mesiodistal space available. Ideally there should be 7.3 mm of interproximal space. If inadequate space is available, consider extraction of all mandibular incisors. Place two 4.0 × 12–mm dental implants in the lateral incisor positions and fabricate a four-unit restoration. Restoration: MCR crown over a one-piece implant | 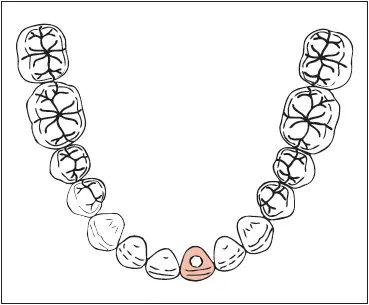 |
| Missing: Maxillary lateral incisor Abutments: Central incisor and canine Considerations: Caries and/or restorations on the abutments would require MCR retainers. If the canine is long, well-supported periodontally, and in need of restoration, and if the pontic will not contact in centric relation or excursions, a single-abutment cantilever fixed partial denture could be used. An untouched central incisor and a first premolar in need of restoration would allow a pontic cantilevered from MCRs on the canine and first premolar. Retainers: Resin-bonded retainers Pontic: Modified ridge lap MCR Abutment-pontic root ratio: 2.6 | 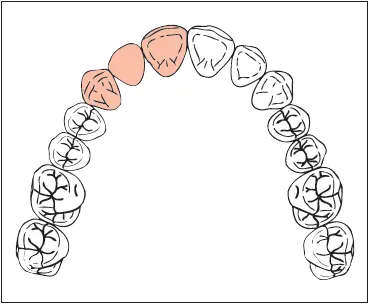 |
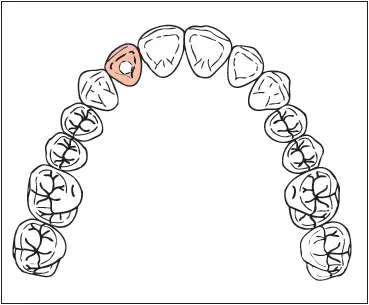 |
Missing: Maxillary lateral incisor Implant: 3.5 × 12 mm Considerations: The loss of a maxillary lateral incisor frequently results in the collapse of the facial plate of bone. The loss of the facial plate of bone often leads to a facial concavity requiring implant placement too far to the lingual. This will result in an unnatural lingual contour of the crown and a poor implant emergence profile. To correct this problem, bone grafting is required to eliminate the facial concavity. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) |
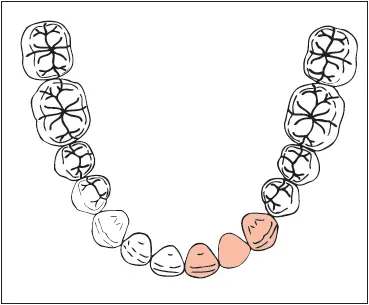 |
Missing: Mandibular lateral incisor Abutments: Central incisor and canine Considerations: An implant-supported MCR is the overriding choice for restoring this space. Caries and/or restorations on the abutments would require MCR crowns and a fixed partial denture. The patient should be warned of the potential for pulpal involvement with resultant endodontic treatment and a dowel core. Double abutting the central incisors for a fixed partial denture would complicate this case immensely. Cantilever fixed partial dentures are not an option for the replacement of mandibular lateral incisors. Severely rotated, malposed, or mobile abutments may contraindicate the use of a fixed partial denture using adjacent teeth as abutments. In such cases, the removal of all of the mandibular incisors would be necessary. The treatment then would be a canine-to-canine fixed partial denture. Retainers: Resin-bonded retainers Pontic: Modified ridge lap MCR Abutment-pontic root ratio: 2.5 |
 |
Missing: Mandibular lateral incisor Implant: 3.3 × 12 mm Considerations: A dental implant is the restoration of choice. The factor limiting replacement of a mandibular lateral incisor with a dental implant is the mesiodistal space available. Ideally there should be 7.3 mm of interproximal space. If inadequate space is available, consider extraction of all mandibular incisors. Place two 4.0 × 12–mm dental implants in the lateral incisor positions and fabricate a four-unit restoration. Restoration: MCR over a one-piece implant |
| Missing: Maxillary first premolar Abutments: Canine and second premolar Considerations: An implant-supported MCR crown would be the restoration of choice. If the canine is unblemished and the second premolar and first molar are restored or will need restoration, a cantilever prosthesis using MCR retainers on the second premolar and first molar is worthy of consideration. A canine-guided occlusal scheme would be necessary to prevent excessive forces on the cantilever pontic. Retainers: MCRs Pontic: Modified ridge lap MCR Abutment-pontic root ratio: 2.1 | 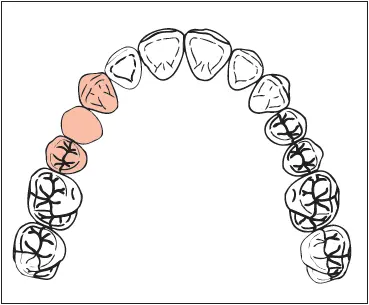 |
| Missing: Maxillary first premolar Implant: 4.0 × 13 mm Considerations: Inadequate facial bone will require bone grafting for dental implant placement. Implant placement may impinge upon the anterior wall of the maxillary sinus. In this event, sinus modification surgery such as sinus grafting or vertical upfracture may be indicated. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) | 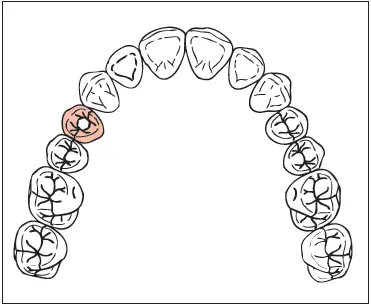 |
| Missing: Mandibular first premolar Abutments: Canine and second premolar Considerations: Facial caries or any proximal caries other than incipient will necessitate MCR retainers. If the canine is intact and the second premolar and first molar are restored or will need restoration, a cantilever fixed partial denture can be used, with MCR retainers on the second premolar and first molar abutments. If the patient does not object, an all-metal crown can be substituted on the molar. Retainers: MCRs Pontic: Modified ridge lap or ovate MCR Abutment-pontic root ratio: 2.5 | 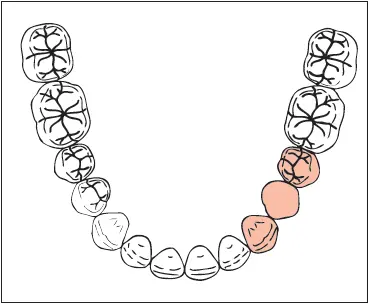 |
 |
Missing: Mandibular first premolar Implant: 4.3 × 11.5 mm Considerations: The position of the anterior loop of the mandibular canal may interfere with implant placement. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) |
 |
Missing : Maxillary second premolar Abutments : First premolar and first molar Considerations : MCR retainers will be required in cases with facial defects such as abfraction or decalcification or when they are requested by the patient. Retainers : MCR on the first premolar and MCR or full coverage gold crown (FGC) on the first molar Pontic : Modified ridge lap MCR Abutment -pontic root ratio: 3.1 |
 |
Missing: Maxillary second premolar Implant: 4.3 × 11.5 mm Considerations: The maxillary sinus will likely interfere with the placement of an implant of desirable length, necessitating sinus modification surgery such as a sinus graft or a vertical upfracture. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) |
| Missing: Mandibular second premolar Abutments: First premolar and first molar Considerations: Esthetic requirements of the patient may necessitate an MCR retainer on the molar. Resin-bonded retainers can be used if the first premolar is large and if the abutments are caries-free or only minimally affected by caries. Retainers: MCR crown on the premolar and FGC on the molar Pontic: Modified ridge lap or ovate MCR Abutment-pontic root ratio: 3.1 | 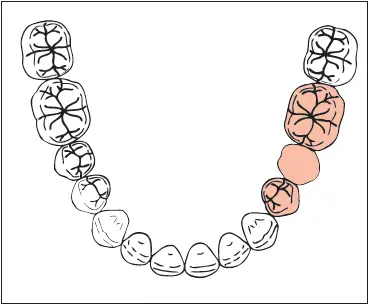 |
| Missing: Mandibular second premolar Implant: 4.3 × 10 mm Considerations: Loss of the facial plate of bone may result in inadequate alveolar width. Alveolar resorption may result in insufficient height of bone above the mental foramen and mandibular canal. The correction of this anatomical difficulty requires the placement of an onlay bone graft to allow the placement of an implant of sufficient width and length. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) | 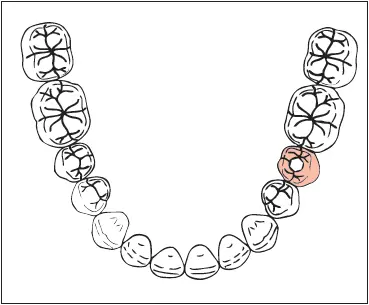 |
| Missing: Maxillary first molar Abutments: Second premolar and second molar Retainers: MCR or ¾ crown on the premolar and ⅞ crown on the molar Pontic: Modified ridge lap MCR Abutment-pontic root ratio: 1.5 | 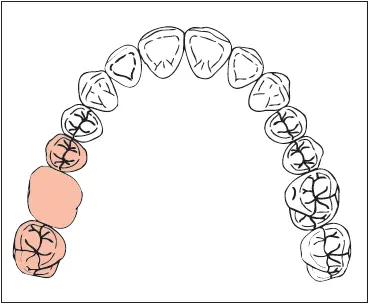 |
 |
Missing: Maxillary first molar Implant: 5.0 × 11.5 mm Considerations: The maxillary sinus will likely interfere with the placement of an implant of desirable length, necessitating sinus modification surgery such as a sinus graft or a vertical upfracture. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) |
 |
Missing: Mandibular first molar Abutments: Second premolar and second molar Considerations: A tilted molar may require orthodontic uprighting, a proximal half crown, or a telescope crown (see chapter 7). Retainers: MCR crown on the premolar and FGC on the molar Pontic: All-metal hygienic, if patient is agreeable. If the patient demands a ceramic occlusal portion, a pontic design that touches the ridge is needed, and metal should extend fully to the ridge to provide rigidity. Abutment-pontic root ratio: 1.5 |
 |
Missing: Mandibular first molar Implant: 5.0 × 10 mm Considerations: Loss of the facial plate of bone may result in inadequate alveolar width. Alveolar resorption may result in insufficient height of bone above the mandibular canal. The correction of this anatomical difficulty requires the placement of an onlay bone graft to allow the placement of an implant of sufficient width and length. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) |
| Missing: Maxillary second molar Considerations: Restoration with a cantilevered fixed partial denture is not recommended due to the excessive tensile stresses placed on the premolar abutment and the retainer. Missing: Maxillary second molar Implant: 5.0 × 11.5 mm Considerations: The maxillary sinus will likely interfere with the placement of an implant of desirable length, necessitating sinus modification surgery such as a sinus graft or a vertical upfracture. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) | 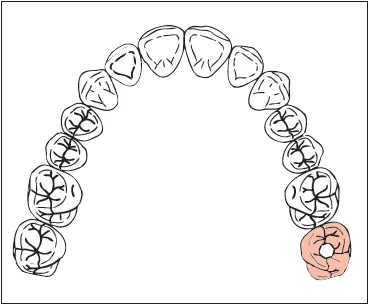 |
| Missing: Mandibular second molar Considerations: Restoration with a cantilevered fixed partial denture is not recommended due to the excessive tensile stresses placed on the premolar abutment and the retainer. Missing: Mandibular second molar Implant: 5.0 × 10 mm Considerations: Loss of the facial plate of bone may result in inadequate alveolar width. Alveolar resorption may lead to insufficient height of bone above the mental foramen and mandibular canal. The correction of this anatomical difficulty requires the placement of an onlay bone graft to allow the placement of an implant of sufficient width and length. Restoration: MCR over a custom abutment (UCLA, Atlantis, or preparable abutment) | 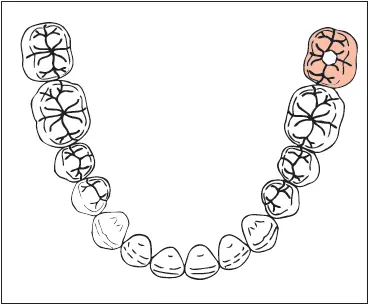 |
Complex Fixed Partial Dentures (One Tooth)
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.