James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
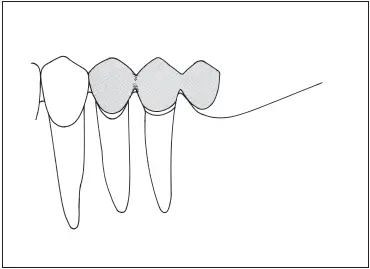
Fig 7-39Cantilever fixed partial denture replacing a mandibular first molar, using both premolars as abutment teeth. To minimize stress on the abutments, the pontic is the size of a premolar rather than a molar.
References
1. Klaffenbach AO. Gnathodynamics. J Am Dent Assoc 1936;23: 371–382.
2. Penny RE, Kraal JH. Crown-to-root ratio: Its significance in restorative dentistry. J Prosthet Dent 1979;42:34–38.
3. Jepsen A. Root surface measurement and a method for xray determination of root surface area. Acta Odontol Scand 1963;21:35–46.
4. Kalkwarf KL, Krejci RF, Pao YC. Effect of apical root resorption on periodontal support. J Prosthet Dent 1986;56:317–319.
5. Tylman SD. Theory and Practice of Crown and Fixed Partial Prosthodontics (Bridge), ed 6. St Louis: Mosby, 1970:17.
6. Johnston JF, Phillips RW, Dykema RW. Modern Practice in Crown and Bridge Prosthodontics, ed 3. Philadelphia: Saunders, 1971:11.
7. Ante IH. The fundamental principles of abutments. Mich State Dent Soc Bull 1926;8:14–23.
8. Nyman S, Lindhe J. Prosthetic rehabilitation of patients with advanced periodontal disease. J Clin Periodontol 1976;3:135–147.
9. Nyman S, Lindhe J, Lundgren D. The role of occlusion for the stability of fixed bridges in patients with reduced periodontal tissue support. J Clin Periodontol 1975;2:53–66.
10. Lindhe J, Nyman S. The role of occlusion in periodontal disease and the biologic rationale for splinting in treatment of periodontitis. Oral Sci Rev 1977;10:11–43.
11. Jacobi R, Shillingburg HT Jr, Duncanson MG Jr. Effect of abutment mobility, site, and angle of impact on retention of fixed partial dentures. J Prosthet Dent 1985;54:178–183.
12. Nyman S, Lindhe J. A longitudinal study of combined periodontal and prosthetic treatment of patients with advanced periodontal disease. J Periodontol 1979;50:163–169.
13. Smyd ES. Mechanics of dental structures: Guide to teaching dental engineering at undergraduate level. J Prosthet Dent 1952;2:668–692.
14. Smyd ES. Advanced thought in indirect inlay and fixed bridge fabrication. J Am Dent Assoc 1944;31:759–768.
15. Dykema RW. Fixed partial prosthodontics. J Tenn Dent Assoc 1962;42:309–321.
16. Rudd KD, O’Leary TJ, Stumpf AJ. Horizontal tooth mobility in carefully screened subjects. Periodontics 1964;2:65–68.
17. Parfitt GJ. Measurement of the physiological mobility of individual teeth in an axial direction. J Dent Res 1960;39:608–618.
18. McCall JO, Hugel IM. Movable-removable bridgework: Principles and practice as developed by Herman ES Chayes, DDS. Dent Items Interest 1949;71:512–525.
19. Shillingburg HT Jr, Fisher DW. Nonrigid connectors for fixed partial dentures. J Am Dent Assoc 1973;87:1195–1199.
20. Standlee JP, Caputo AA. Load transfer by fixed partial dentures with three abutments. Quintessence Int 1988;19:403–410.
21. Markley MR. Broken-stress principle and design in fixed bridge prosthesis. J Prosthet Dent 1951;1:416–423.
22. Sutherland JK, Holland GA, Sluder TB, White JT. A photoelastic analysis of the stress distribution in bone supporting fixed partial dentures of rigid and nonrigid design. J Prosthet Dent 1980;44:616–623.
23. Landry KE, Johnson PF, Parks VJ, Pelleu GB Jr. A photoelastic study to determine the location of the nonrigid connector in a five-unit intermediate abutment prosthesis. J Prosthet Dent 1987;57:454–457.
24. Picton DC. Tilting movements of teeth during biting. Arch Oral Biol 1962;7:151–159.
25. Khouw FE, Norton LA. The mechanism of fixed molar uprighting appliances. J Prosthet Dent 1972;27:381–389.
26. Norton LA, Profitt WR. Molar uprighting as an adjunct to fixed prostheses. J Am Dent Assoc 1968;76:312–315.
27. Simon RL. Rationale and practical technique for uprighting mesially inclined molars. J Prosthet Dent 1984;52:256–259.
28. Norton LA, Parker WT. Management of repositioned teeth in preparation for fixed partial dentures. J Am Dent Assoc 1970; 81:916–922.
29. Reynolds JM. Abutment selection for fixed prosthodontics. J Prosthet Dent 1968;19:483–488.
30. Hood JA, Farah JW, Craig RG. Modification of stresses in alveolar bone induced by a tilted molar. J Prosthet Dent 1975;34:415– 421.
31. Yang HS, Thompson VP. A two-dimensional stress analysis comparing fixed prosthodontic approaches to the tilted molar abutment. Int J Prosthodont 1991;4:416–424.
32. Smith DE. Fixed bridge restorations with the tilted mandibular second or third molar as an abutment. J South Calif Dent Assoc 1939;6:131–138.
33. Shillingburg HT Jr. Bridge retainers for tilted abutments. N M Dent J 1972;22:16–19.
34. Ewing JE. Re-evaluation of the cantilever principle. J Prosthet Dent 1957;7:78–92.
35. Wright KW, Yettram AL. Reactive force distributions for teeth when loaded singly and when used as fixed partial denture abutments. J Prosthet Dent 1979;42:411–416.
36. Wright WE. Success with the cantilever fixed partial denture. J Prosthet Dent 1986;55:537–539.
37. Goldfogel MH, Lambert RL. Cantilever fixed prosthesis replacing the maxillary lateral incisor: Design consideration. J Prosthet Dent 1985;54:477–478.
38. Schweitzer JM, Schweitzer RD, Schweitzer J. Free-end pontics used on fixed partial dentures. J Prosthet Dent 1968;20:120–138.
39. Nyman S, Lindhe J. Considerations on the design of occlusion in prosthetic rehabilitation of patients with advanced periodontal disease. J Clin Periodontol 1977;4:1–15.
Table 7-1 Types of prostheses used for the replacement of missing teeth
| Removable partial denture | Conventional tooth-supported fixed partial denture | Resin-bonded tooth-supported fixed partial denture | Implant-supported fixed partial denture | |
|---|---|---|---|---|
| Span length | Posterior spans longer than 2 teeth Anterior spans longer than 4 incisors Canine + 2 or more contiguous teeth | Posterior span: 2 or fewer Incisors: 4 or fewer | Single tooth Possible for 2 incisors | Single tooth 2- to 6-unit span |
| Span configuration | No distal abutment Multiple or bilateral edentulous spaces | Usually has distal abutment but can be used with short cantilever pontic | Abutments mesial and distal to pontic | No distal abutment Pier in 3+ pontic span All abutments at ends and as pier(s) of long span |
| Abutment alignment | Tipped abutments can be tolerated Widely divergent abutment alignment | Less than 25-degree inclination can be accommodated by preparation modification | Less than 15-degree inclination mesiodistally Should be in same faciolingual plane Preparations are not easily modified because of minimal reduction | Need for implant/abutment alignment requires close coordination between surgeon and restorative dentist |
| Abutment condition | Short clinical crownsInsufficient abutments | Good if abutments need crowns Nonvital teeth can be used if there is sufficient coronal tooth structure | Defect-free abutments Incisor, premolar replacements | Defect-free abutments requiring no restoration |
| Occlusion | More adaptable to irregularities in a healthy opposing natural dentition | Favorable loading (magnitude, direction, frequency, duration) | Cannot be used for incisor replacement in presence of deep vertical overlap | Occlusal forces must be as nearly vertical as possible to prevent unfavorable lateral loading of implants |
| Periodontal condition | Can use alternate (secondary) abutments when primary abutments are weakened | Good alveolar bone support Crown-root ratio 1:1 or better No mobility Favorable root morphology Provides rigid stabilization | No mobility Periodontal splints (with auxiliary resistance in tooth preparation) | Dense bone |
| Ridge form | Gross tissue loss in residual ridge | Moderate resorption No gross soft tissue defects | Moderate resorption No gross soft tissue defects | Broad, flat ridge |
| General features | Dry mouth: poor prognosis Limited patient finances Acceptable oral hygiene Reliable recall candidate Treatment simplification Advanced age Systemic health problems More adaptable to dentition in transition to edentulous state | Dry mouth: high caries risk Muscular discoordination Mandibular tori Palatal soft tissue lesions Large tongue Exaggerated gag reflex Unfavorable attitude toward RPD Patient can’t cope with aging, tooth loss Favorable opposing occlusion: removable prosthesis or periodontally weakened natural dentition may permit FPD in less than optimal situations Must be within dentist’s skills | Well suited for young patients Can be used for replacing molars if masticatory muscles are not too well developed | Able to survive in dry mouth May be better choice if teeth will require extensive treatment and will still be weak, questionable abutments Unfavorable attitude toward RPD Must be within dentist’s skills |
RPD, removable partial denture; FPD, fixed partial denture.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.