Tomas Linkevičius - Zero Bone Loss - Knochenerhaltende Behandlungskonzepte
Здесь есть возможность читать онлайн «Tomas Linkevičius - Zero Bone Loss - Knochenerhaltende Behandlungskonzepte» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на немецком языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Zero Bone Loss: Knochenerhaltende Behandlungskonzepte
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Zero Bone Loss: Knochenerhaltende Behandlungskonzepte: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Zero Bone Loss: Knochenerhaltende Behandlungskonzepte»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Der Autor ist fest davon überzeugt, dass sich der Knochen mithilfe verschiedener chirurgischer und prothetischer Lösungen stabilisieren lässt und zieht dafür nicht nur klinische Befunde und Fallberichte, sondern überwiegend kontrollierte klinische Studien und sorgfältig geplante In-vitro-Studien heran. Damit erhält der Leser mit diesem Buch genau das, was er benötigt: klinische Verfahren, die durch solide klinische Evidenz gestützt werden.
Zero Bone Loss: Knochenerhaltende Behandlungskonzepte — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Zero Bone Loss: Knochenerhaltende Behandlungskonzepte», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
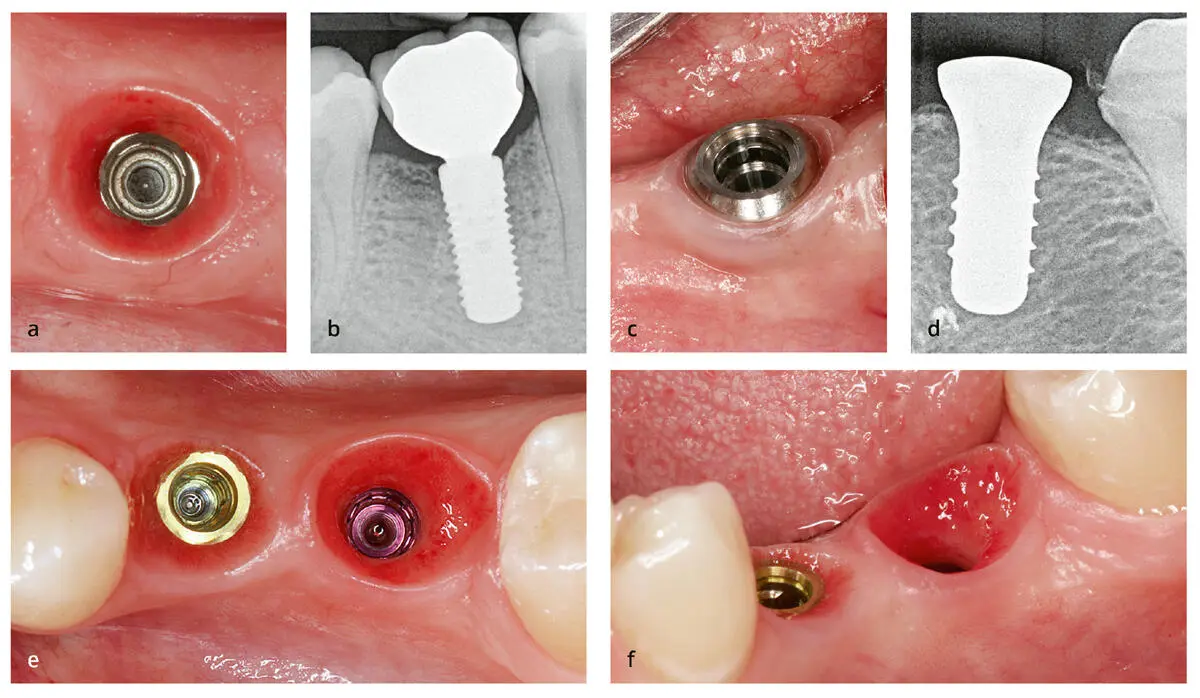
Abb. 3-16Aus prothetischer Sicht ist der klinische Unterschied zwischen Implantaten auf Gewebe- und auf Knochenniveau offensichtlich. (a) Bei einem Implantat auf Knochenniveau hat das Weichgewebe Kontakt mit der Restauration. (b) Kontakt zwischen Weichgewebe und der Zirkonoxidrestauration. (c) Ein Implantat auf Gewebeniveau ist vollständig von Weichgewebe umgeben. (d) Das Weichgewebe hat auf gesamter Höhe nur Kontakt mit dem polierten Titanhals. (e und f) Das für die Restauration zur Verfügung stehende Weichgewebe unterscheidet sich erheblich zwischen dem Implantat auf Gewebeniveau (links) und dem Implantat auf Knochenniveau (rechts) .
Zusammenfassung
Implantate auf Knochenniveau ohne Platform-Switching sollten einen etwa 1 mm langen maschinierten Hals besitzen und leicht suprakrestal gesetzt werden, damit der Mikrospalt und die damit einhergehenden Bakterien Abstand zum Knochen haben. In dieser Position ist die Stabilität der Implantat-Abutment-Verbindung weniger wichtig. Bewegungen sind nicht so verheerend für den Knochen, weil sie in einem sicheren vertikalen Abstand auftreten.
Implantate mit Platform-Switching können auf oder unter Knochenniveau gesetzt werden. Die Tiefe hängt von der Stabilität der Implantat-Abutment-Verbindung ab.
Implantate auf Gewebeniveau müssen so gesetzt werden, dass der polierte Implantathals vollständig aus dem Knochen ragt. Abhängig von der vertikalen Dicke der Weichgewebe kann die Verwendung von Implantaten auf Gewebeniveau die Wahl des prothetischen Materials für die Restauration einschränken.
Literatur
1.Berglundh T, Gotfredsen K, Zitzmann NU, Lang NP, Lindhe J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: An experimental study in dogs. Clin Oral Implants Res 2007;18:655–661.
2.Lang NP, Berglundh T; Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: Where are we now?—Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol 2011;38(suppl 11):178–181.
3.Esposito M, Ardebili Y, Worthington HV. Interventions for replacing missing teeth: Different types of dental implants. Cochrane Database Syst Rev 2014;(7): CD003815.
4.Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and/or surface topography on biofilm development. Clin Oral Implants Res 2006;17(suppl 2):68–81.
5.Heitz-Mayfield LJ, Mombelli A. The therapy of periimplantitis: A systematic review. Int J Oral Maxillofac Implants 2014;29(suppl):325–245.
6.Keeve PL, Koo KT, Ramanauskaite A, et al. Surgical treatment of periimplantitis with non-augmentative techniques Implant Dent 2019;28(2):177–186.
7.Ketabi M, Deporter D. The effects of laser microgrooves on hard and soft tissue attachment to implant collar surfaces: A literature review and interpretation. Int J Periodontics Restorative Dent 2013;33:e145–e152.
8.Nevins M, Kim DM, Jun SH, Guze K, Schupbach P, Nevins ML. Histologic evidence of a connective tissue attachment to laser microgrooved abutments: A canine study. Int J Periodontics Restorative Dent 2010;30:245–255.
9.Abdallah MN, Badran Z, Ciobanu O, Hamdan N, Tamimi F. Strategies for optimizing the soft tissue seal around osseointegrated implants. Adv Healthc Mater 2017;6. doi:10.1002/adhm.201700549.
Конец ознакомительного фрагмента.
Текст предоставлен ООО «ЛитРес».
Прочитайте эту книгу целиком, купив полную легальную версию на ЛитРес.
Безопасно оплатить книгу можно банковской картой Visa, MasterCard, Maestro, со счета мобильного телефона, с платежного терминала, в салоне МТС или Связной, через PayPal, WebMoney, Яндекс.Деньги, QIWI Кошелек, бонусными картами или другим удобным Вам способом.
Интервал:
Закладка:
Похожие книги на «Zero Bone Loss: Knochenerhaltende Behandlungskonzepte»
Представляем Вашему вниманию похожие книги на «Zero Bone Loss: Knochenerhaltende Behandlungskonzepte» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Zero Bone Loss: Knochenerhaltende Behandlungskonzepte» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.