Mario Roccuzzo - Peri‑Implant Soft‑Tissue Integration and Management
Здесь есть возможность читать онлайн «Mario Roccuzzo - Peri‑Implant Soft‑Tissue Integration and Management» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Peri‑Implant Soft‑Tissue Integration and Management
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Peri‑Implant Soft‑Tissue Integration and Management: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Peri‑Implant Soft‑Tissue Integration and Management»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Peri‑Implant Soft‑Tissue Integration and Management — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Peri‑Implant Soft‑Tissue Integration and Management», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
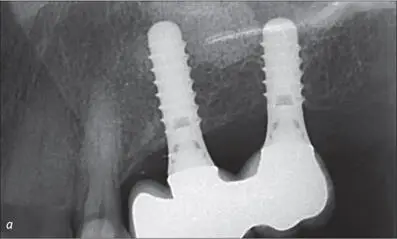
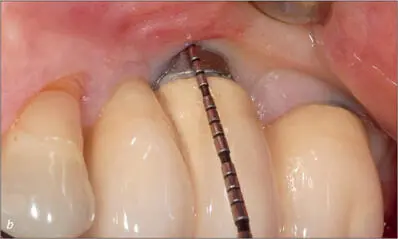
Fig 10a-b Radiographic and clinical view of two implants (SLA S, diameter 4.1 mm, length 12 mm, and S, diameter 4.1 mm, length 10 mm; Institut Straumann AG), placed two years previously into a thin ridge, presenting with an inferiorly attaching frenulum facially to implant 26. Treatment was indicated to facilitate plaque control and to prevent further progression of the recession.
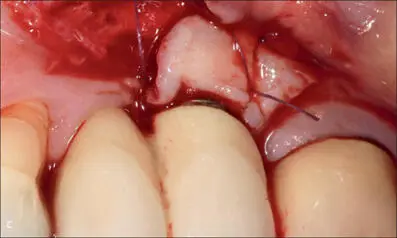

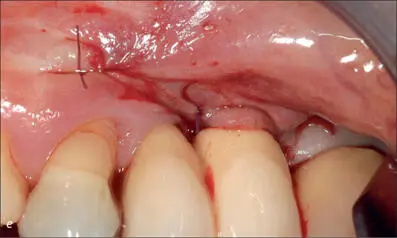
Fig 10c-e A trapezoidal split-thickness flap was elevated at the implant site. A connective-tissue graft was adapted and placed in a fully submerged approach for optimal blood supply.

Fig 10f Nine years after the surgical correction. Plaque control was improved around the treated mesial implant, while the soft-tissue dehiscence had increased on the distal implant, which had not received further treatment. The surgical trauma, the shallow vestibule, the lack of keratinized attached mucosa or a thin buccal bone plate at the crestal level may have contributed to the formation of the dehiscence/recession at the most distally located implant.
While a pocket depth of 5 mm with bleeding on probing around a tooth is, by definition, pathological, the same cannot be said if found around an implant. Around dental implants, the AAP/EFP workshop suggested that it is not currently possible to determine what constitutes a physiological pocket depth (Schwarz and coworkers 2018; Berglundh and coworkers 2018). It is hard to clearly assess, during supportive care, when a peri-implant pocket should be considered excessive and would require treatment.
Two recent studies have tried to investigate the correlation between peri-implant pocket depths and bleeding.
Merli and coworkers (2017) analyzed 92 implants and found bleeding in 39% of the sites. The odds ratio increased by 1.81 (95%-CI, 1.47–2.23; p < 0.0001) for each 1-mm increment in pocket depth. The authors concluded that the probability of peri-implant bleeding on probing was positively associated with peri-implant pocket depth.
Similar findings were reported by Farina and coworkers (2017), who tried to identify factors associated with the probability of peri-implant bleeding on probing in 112 patients, with data related to 1,725 peri-implant sites. The results of the study indicated that the odds ratio increased by 1.6 for each 1-mm increment in pocket depth. Since the deeper the pocket, the higher the probability of bleeding, clinicians should make every effort to control pocket depths around implants during supportive care, even in the absence of any evidence of biological complications.
Moreover, in selected circumstances, surgical modification of the soft tissue is advisable to reduce the depth of the peri-implant mucosal tunnel, particularly if concomitant bleeding is found, as in the case of the 64-year-old man presented in Figures 11a-f.
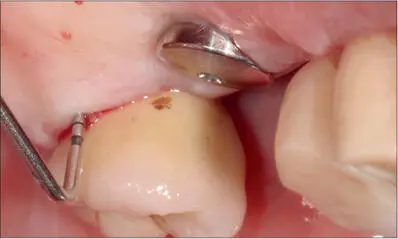
Fig 11a Implant 27, placed nine years previously, palatal view. 13-mm pocket and bleeding on probing. Implant 26 had been placed recently and not yet been loaded. The deep pocket at implant 27 should have been addressed before placing the new implant, or at least at the same time.
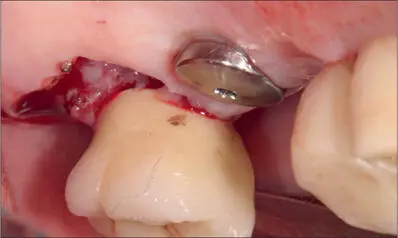
Fig 11b Gingivectomy to eliminate the excessive soft tissue.

Fig 11c Application of a periodontal dressing.

Fig 11d Early healing six weeks after surgery.
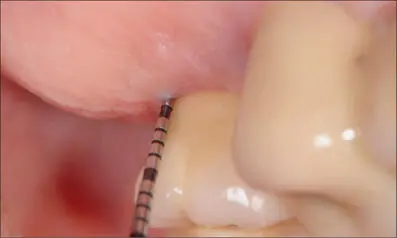
Fig 11e Palatal view of implant 27, presenting with 3-mm probing depth and no bleeding.
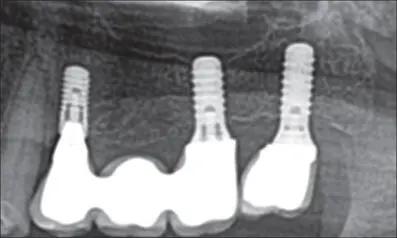
Fig 11f Panoramic radiograph. Ideal peri-implant bone levels around the distal implant at the fifteen-year follow-up.
The main objectives in treating peri-implantitis are:
• decontamination of the implant surface
• removal of infected/inflamed tissue
• creation of a soft-tissue architecture to facilitate oral hygiene.
To achieve this, it is often necessary to elevate a full-thickness flap to remove the granulation tissue resulting from the local inflammation and to decontaminate the implant surface. Depending on the configuration of the defect, a reconstructive approach is often preferred, with or without a membrane. One of the possible negative outcomes of this approach is the creation of a peri-implant soft-tissue dehiscence (Heitz-Mayfield and coworkers 2018a; Roccuzzo and coworkers 2017a). If such a dehiscence raises esthetic concerns, particularly in patients with high esthetic expectations, additional interventions may be required (see Chapter 5.2, Fig 3).
To reduce the need for multiple surgery, particularly if a soft-tissue dehiscence is already present, the surgical treatment of peri-implantitis may be accompanied by the application of a connective-tissue graft (CTG) (Roccuzzo and coworkers 2016). Figures 12a-yillustrate a case where the surgical treatment of a peri-implantitis defect was associated with the application of a CTG.
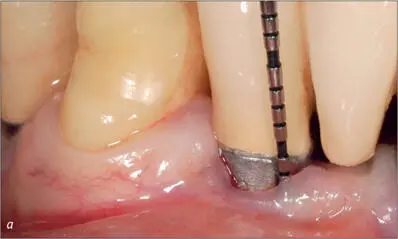
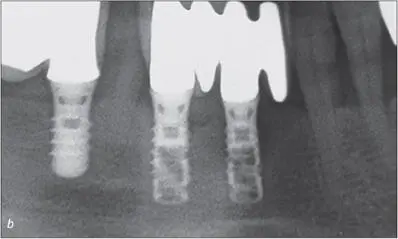
Fig 12a-b Radiographic and clinical view of a hollow-screw implant placed in November 1994, presenting with a pocket and a soft-tissue dehiscence.
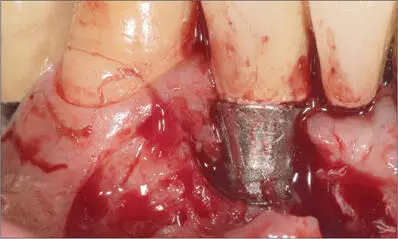
Fig 12c After raising a full-thickness flap, the granulation tissue was removed with a titanium brush and curettes.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Peri‑Implant Soft‑Tissue Integration and Management»
Представляем Вашему вниманию похожие книги на «Peri‑Implant Soft‑Tissue Integration and Management» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Peri‑Implant Soft‑Tissue Integration and Management» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.