Irena Sailer - Fixed Restorations
Здесь есть возможность читать онлайн «Irena Sailer - Fixed Restorations» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fixed Restorations
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fixed Restorations: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fixed Restorations»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The book is divided into four parts: basic information regarding materials and production processes, step-by-step clinical procedures with extensive case presentations, long-term outcomes, and management of complications. With over 2000 clinical images and diagrams, backed up with the scientific evidence for recommendations, the best practice for tooth- and implant-supported fixed restorations is clearly described. The vast clinical and technical knowledge and experience of the authors has resulted in a unique textbook that will aid in decision making regarding material selection and procedures for all patients in need of fixed restorations.
Fixed Restorations — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fixed Restorations», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The third and last time point to determine the desired restoration design is after the final impression is performed and before the framework is produced. The patient’s and restorative team’s impression derived from the previous two diagnostic steps (diagnostic mock-up and provisional phase) are thereby taken into consideration, and a new tentative configuration is confectioned over the prepared abutments on the final cast. Using tooth-colored wax, the technician produces a wax try-in that will simulate the color and contour of the final restoration. When the case involves edentulous spans or multiple units, the wax structure can require a metal or resin framework to improve its strength. An advantage of this diagnostic maneuver lies in the plasticity of the wax, which allows for immediate modifications of possible imperfections discussed during the try-in appointment. Once the patient and the restorative team have agreed on the optimal restorative outline, the wax try-in will be used as a reference to determine the shape and thickness of framework and veneering of the final restoration.
1.4.4 Conventional procedures
As previously mentioned, high efforts are devoted to identify and mimic the desired esthetic outcome before the technician begins the final restoration production. Despite the significant amount of energy and time invested to come up with a diagnostic draft, the obtained result may not match the patient’s physiognomy or personality, or it may not represent the desired result the restorative team and the patient expected. In these cases, small changes to modify this initial draft can be attempted. However, the range of modifications is limited and often a new diagnostic version is necessary. The inability to achieve the expected esthetic diagnosis with a try-in leads to patient dissatisfaction and, even worse, professionals’ frustration and increased time and economic expenses since further diagnostic steps are necessary.
1.4.5 Digital procedures
In order to overcome the abovementioned limitations new computerized technology procedures may be helpful. Computer technology is increasingly transforming the way dentistry is being performed. CAD/CAM processes are transforming what were previously manual tasks into easier, faster, cheaper, and more predictable mechanized methods 9. Current industrial product development would be impossible without CAD technologies. No engineer would consider designing a prototype layering or carving a structure manually; instead a virtual environment is used, where different versions can be tried-in without increasing significantly the time invested and with no impact on the costs. Carving shapes manually has evolved into designing volumes virtually by means of dedicated software. In restorative dentistry, the wax and modeling are evolving into software and mouse-clicks. The restorative team can profit from virtual libraries from where different tooth morphologies can be selected (Exocad, Darmstadt, Germany; 3Shape A/S; Copenhagen, Denmark; Dental Wings, Montreal, Canada; Sirona Dental, Wals, Austria). These software tools offer a high number of different tooth shapes categorized according to parameters such as size, age, or patient’s phenotype. Moreover, real teeth can be used as a reference to generate tooth morphology proposals 10. These standard shapes can later be modified and adapted to individual patient situations. Working time is substantially reduced by eliminating the manual work needed for conventional waxing techniques. This allows the technician to focus solely on shapes and tooth arrangements. Furthermore, certain software enable us to integrate photorealistic 3D restorations of the patients’ face into the virtual design software 11. The face is integrated by means of two-dimensional (2D) digital photographs projected onto a three-dimensional (3D) virtual skull or by means of 3D facial scanners. This allows for virtual smile design, taking into consideration important facial reference planes such as midline verticality, smile line, or the true horizontal plane. A further benefit is the possibility to rapidly modify an initial design version in order to effortlessly try-in other tooth arrangements. This grants the technician freedom to generate multiple versions of the future restoration in an efficient manner. Being able to offer different versions at a single appointment streamlines the diagnostic phase and potentially better fulfills the wishes of the most demanding patients and clinicians.
So far, subtractive CAM processes dominate dental manufacturing routines. Restorations are obtained by trimming a solid block of material into the desired 3D object, by means of a computer-controlled milling machine 12. However, these procedures present several shortcomings such as waste of considerable amounts of material, impossibility to create geometries that lie below the milling bur diameter, or the impossibility to allow for mass production of components 9 , 13. These restrictions can be overcome by the introduction of additive processing routes of layered fabrication 14. An example of these technologies is 3D printers, which allow the manufacturing of several objects at the same time in a precise and cost-efficient manner. The 3D printers work by jetting to be photopolymerized materials in ultrathin layers. Each layer is cured by ultraviolet light immediately after it is deposited, producing fully cured objects 15. The dual jetting printing procedure requires two materials: a hard, fundamental material, and a gel-like support material. The support material is necessary to sustain complex geometries of the fundamental material during fabrication and it is easily removed by water jetting after printing. Micron-accurate shapes can be printed in different combinations of photopolymers, producing materials with specific mechanical and visual properties. Products with different levels of strength, rigidity, color, transparency, heat resistance, or texture can be obtained. This production modality has widened the indication spectrum of restorative computer-assisted dentistry.
In the following, a computer-assisted diagnostic treatment sequence will be described in detail and clinical examples given to illustrate the recent options for virtual diagnostics and CAD/CAM mock-ups (Fig 1-4-1).
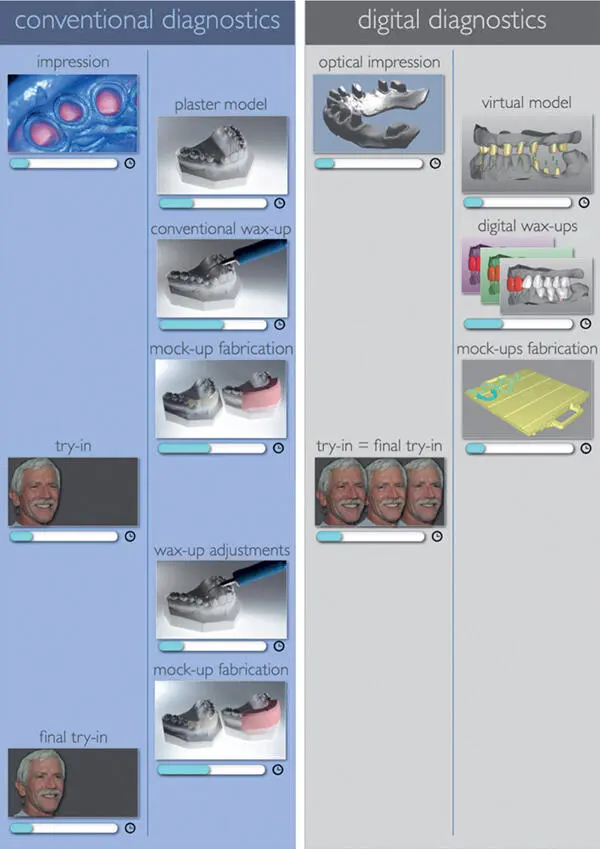
Fig 1-4-1 Comparison of conventional and digital workflows for diagnostics (reproduced from Sancho-Puchades et al 16, with permission).
The anatomical data acquisition of the patient’s jaws can be obtained either by direct capturing the volumetric information using intraoral optical scanners or by digitalizing a plaster model by a laboratory optical scanner 17(Figs 1-4-2 and 1-4-3).
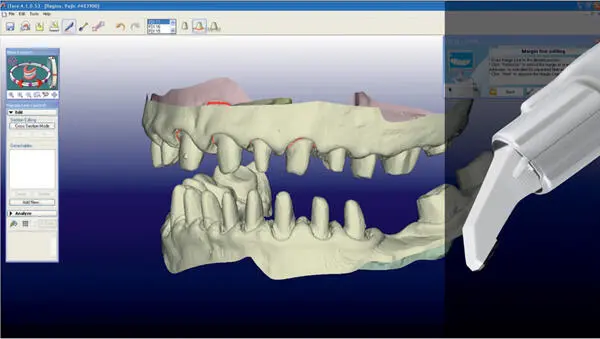
Fig 1-4-2 Optical impression of patient situation (reproduced from Sancho-Puchades et al 16, with permission).
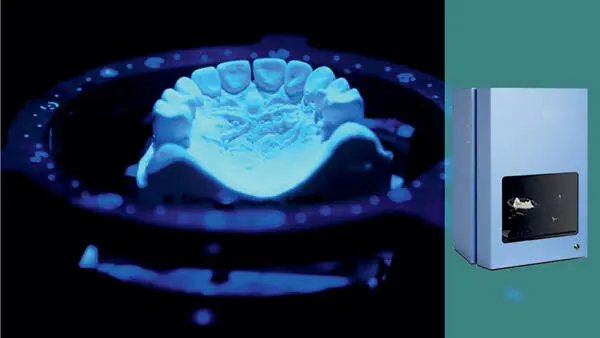
Fig 1-4-3 Scan of stone case in the laboratory with a laboratory scanner (reproduced from Sancho-Puchades et al 16, with permission).
The .STL data generated is transferred into a software package that allows for virtual dental restoration design. After selecting the abutment teeth to reconstruct, a specific tooth shape set is chosen from the virtual tooth library. The projected tooth forms are manually arranged by the dental technician onto the dental arch (Fig 1-4-3). Variations on the mesiodistal, buccooral, and occlusogingival dimensions, tooth axis, or tooth composition can be easily performed with the design software. Once a first version is completed and saved on the computer, modifications of the first design can be efficiently created with a couple of clicks and saved as new versions. For example, a standard tooth arrangement can easily be individualized by intruding or rotating teeth simply dragging a virtual point.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fixed Restorations»
Представляем Вашему вниманию похожие книги на «Fixed Restorations» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «Fixed Restorations» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.