Lynelle R. Johnson - Canine and Feline Respiratory Medicine
Здесь есть возможность читать онлайн «Lynelle R. Johnson - Canine and Feline Respiratory Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Canine and Feline Respiratory Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Canine and Feline Respiratory Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Canine and Feline Respiratory Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
includes more detail and new information throughout, particularly in the areas of antimicrobial guidelines, anti-fungal therapies, and ant-viral medications in cats.
Logically organized for ease of use in the practice setting,
features problem-based learning to enhance working knowledge of the topics discussed. Chapters cover localization of disease, respiratory diagnostics, respiratory therapeutics, nasal disorders, and diseases of airways. Sections on parenchymal disease; pleural and mediastinal disease; and vascular disorders are also presented.
Offers a complete guide to the diagnosis and treatment of respiratory conditions in canine and feline patients—now expanded to include more detailed and advanced information Focuses on localization of disease, diagnostic testing, and appropriate therapy Thoroughly updated with new antimicrobial guidelines, the latest information on anti-fungal therapy, and new advances in ant-viral medications in cats Includes many new images and topics for discussion Features problem-based learning to support a working understanding of the topics discussed
is an essential resource for veterinary internal medicine specialists, general practitioners, and veterinary students.
Canine and Feline Respiratory Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Canine and Feline Respiratory Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:

Figure 2.16 A periodontal probe is inserted along the gum lines surrounding each tooth after imaging and rhinoscopy have been completed. Pockets > 1 mm depth in the cat and > 2–3 mm depth in the dog could result in clinically significant nasal disease due to tracking of bacteria up the tooth root into the nasal cavity.
Laryngoscopy
Laryngoscopy can be performed as an isolated procedure or during the preliminary assessment of the airway before a transoral tracheal wash or bronchoscopy. An appropriate anesthetic protocol must be devised that provides a light plane of anesthesia and preserves laryngeal function. While multiple agents are appropriate for use, the key feature is to have spontaneous and vigorous respirations. An assistant is required to identify thoracic inspiratory efforts so that the examiner can insure coordination of laryngeal abduction with inspiration. If the plane of anesthesia is too deep, one to two boluses of doxapram (0.5–1.0 mg/kg) can be used to stimulate respirations (Miller et al. 2002). An accurate laryngeal examination is important because laryngeal dysfunction can be a contributing component to cough in up to 20% of dogs, even when signs of upper airway disease are lacking (Johnson 2016).
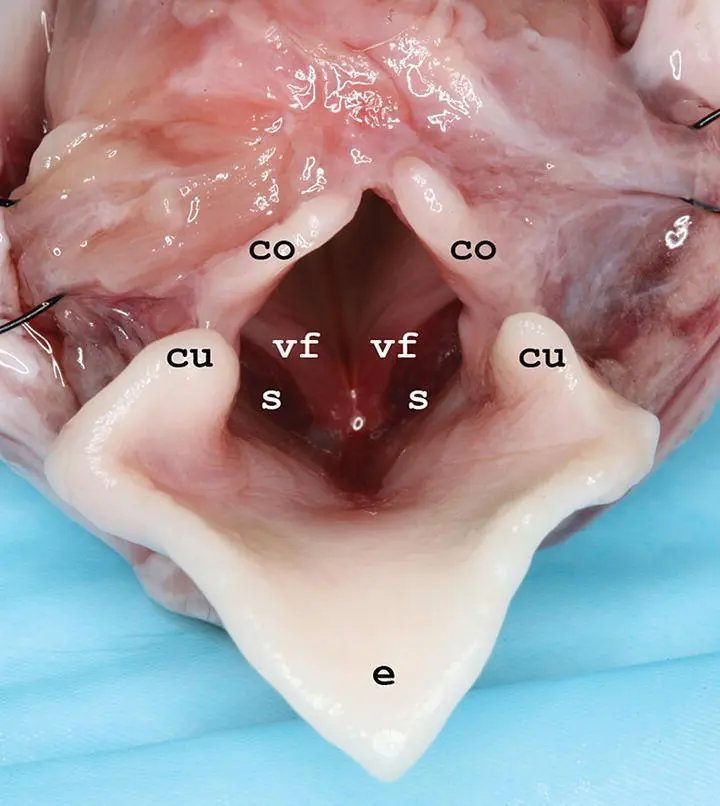
Figure 2.17 Necropsy image of the larynx showing the corniculate processes of the arytenoids (co), vocal folds (vf), cuneiform processes of the arytenoids (cu), saccules (s), and epiglottis (e).
Laryngoscopy includes the assessment of function as well as examination of all structures in the area of the rima glottis, including the soft palate, tonsils, laryngeal aditus, and saccules ( Figure 2.17). The larynx is inspected for edema, hyperemia, or accumulation of secretions, any of which could indicate injury due to turbulent airflow, acid reflux, or lower airway inflammation. Eversion of laryngeal saccules is a common contributor to obstruction to airflow in the upper airways (see Chapter 4). Because they are membranous tissue, saccules are very responsive to manipulation and can become more swollen as the upper airway evaluation continues, so it is important not to over‐interpret this finding. In the normal dog, the soft palate should not overlap with the epiglottis by more than a few millimeters. Tonsils should be within their crypts; enlargement or eversion is suggestive of inflammation or irritation.
Bronchoscopy
Bronchoscopy is one of the most useful techniques for providing a diagnosis in animals with airway or lung disease. It can define the location, grade, and extent of tracheal ring flattening for planning stabilization through surgery or stent implantation, identify protrusion of the dorsal tracheal membrane into the tracheal lumen, document tracheal inflammation or irritation, visualize intrathoracic bronchial or airway collapse, and allow collection of BAL fluid to determine the contribution of small airway disease to respiratory signs. It is also highly useful and successful in managing foreign body inhalation.
Complications that can be encountered after bronchoscopy are worsened cough or increased airway obstruction. These occur most commonly in dogs that have severe tracheal collapse or bronchomalacia, because irritation of the airway potentiates a cough, and suppression of respiratory effort by anesthetic agents allows passive collapse of diseased large and small airways. Excessive stress that induces cough and respiratory distress during recovery is particularly troublesome. Coughing can be partly alleviated by administering dilute lidocaine (approximately 1 ml of 1% lidocaine for a small dog) through the bronchoscope into the trachea at the end of the procedure. Subcutaneous terbutaline (0.01 mg/kg) may improve respirations in dogs with collapsed airways (although it does not act as a bronchodilator in this situation), and recovery in an oxygen‐enriched environment can lessen respiratory distress. Bronchospasm can be a particular problem in the cat with inflammatory airway disease that has severe cough and respiratory distress. Terbutaline should be given subcutaneously immediately prior to the procedure at 0.01 mg/kg to produce airway smooth muscle relaxation and reduce complications. Aerosolized albuterol can be given through the endotracheal tube at the end of the procedure if injectable terbutaline is not available.
General anesthesia is required during bronchoscopy to suppress coughing and laryngospasm, to allow examination of the airways without inducing trauma, and to protect the endoscope. Bronchoscopy can be performed using gas anesthesia if the animal is large enough for a 7–8 mm endotracheal tube. A special T adapter is used to pass the scope through the endotracheal tube while administering anesthetic gas and venting expired gases ( Figure 2.18). In small dogs and cats, jet ventilation is typically used to provide oxygenation through bulk flow, because placement of the scope through a small endotracheal tube would lead to airway obstruction and accumulation of CO 2. As an alternative, oxygen can be supplied to the patient using a red rubber catheter attached to the oxygen supply. The catheter should terminate in the distal trachea to avoid the possibility of wedging it into a bronchus and causing airway rupture.
Virtually all animals undergoing bronchoscopy suffer respiratory embarrassment. Prior to bronchoscopy, patients are preoxygenated with a facemask, and an anesthetic protocol is chosen that avoids excessive cardiopulmonary depression. Animals are placed in sternal recumbency and two mouth gags are in place throughout the procedure to protect the bronchoscope. The normal trachea appears round to oval, with minimal laxity in the dorsal tracheal membrane ( Figure 2.19). At the carina, bifurcation in the left and right mainstem bronchi provides a reliable landmark for assessing location within the airways ( Figure 2.20). Normal airways appear round to oval in shape, demonstrate little change in shape or diameter throughout respiration, have minimal secretions, and are pale pink in color ( Figure 2.21). All accessible airways should be evaluated and abnormal regions with mucosal hyperemia or irregularity or areas with mucus accumulation should be identified as possible sites for BAL. If an obviously abnormal site is not visualized, the right middle lobe or caudal portion of the left cranial lobe is often a worthwhile site to lavage, because they are both ventrally oriented and tend to accumulate secretions.

Figure 2.18 A bronchoscopy adapter allows passage of a 5.0 mm endoscope through an endotracheal tube while oxygen and anesthetic gas are administered through the side port.

Figure 2.19 Endoscopic view of the normal canine trachea.
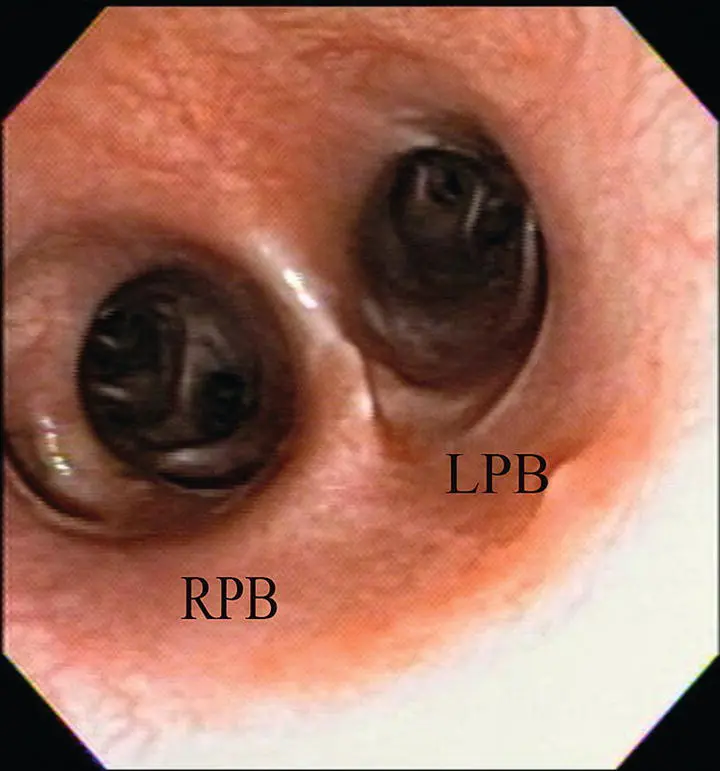
Figure 2.20 Endoscopic view of the carina illustrating the openings into the right principal bronchus (RPB) and left principal bronchus (LPB).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Canine and Feline Respiratory Medicine»
Представляем Вашему вниманию похожие книги на «Canine and Feline Respiratory Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Canine and Feline Respiratory Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.