Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
AFAST with an assigned AFS should continue during patient rounds every 12–24 hours or during recheck examination until ascites resolution, that is, AFS returns to 0, negative.
In questionable or unstable patients, serial AFAST with an assigned AFS are performed as often as necessary. The Global FAST approach is important to rule in and rule out other internal sites of bleeding and comorbidities in the thorax, including heart and lung.
Large‐Volume AFS 3 and 4 Bleeders (AFS ≥3)
In general, postinterventional bleeding in noncoagulopathic patients will not stop without a surgical intervention, in other words, the ligation of the bleeder(s). Many “large‐volume bleeders” are not initially anemic in the acute setting because patients can compensate, especially dogs which have a unique large splenic blood reservoir.
AFS 3 and 4 (modified AFS system ≥3) initially or on serial examinations are “large‐volume bleeders” and in general should be explored or have another appropriate intervention to stop the bleeding as soon as possible, with the caveat that the patient has an acceptable coagulation profile.
The author follows the axiom “If it's an AFS of 3 or 4, you should explore (surgically intervene),” with the caveat that the patient has an acceptable coagulation profile.
Pearl:Waiting on a compensated postinterventional noncoagulopathic “large‐volume bleeder” (AFS ≥3) instead of surgically addressing the cause of bleeding often leads to increased morbidity and cost (e.g., transfusion products) and increased patient anesthetic risk, because “large‐volume bleeders” predictably become markedly to severely anemic and overtly decompensate in time. Thus, “If it's an AFS of 3 or 4, you should explore (surgically intervene),” with the caveat that the patient has an acceptable coagulation profile.
Nontrauma
Nontraumatic hemoabdomen requires a more cerebral approach and knowledge base. Coagulopathy should always be ruled out, including minimally performing basic testing of prothrombin time (PT), activated partial thromboplastin time (aPTT), and a buccal mucosal or nail clip bleed time (platelet function test), readily available onsite tests at most practices. In coagulopathic cases, the coagulopathy generally needs to be corrected before invasive procedures. In noncoagulopathic cases, a bleeding mass is most common in dogs and cats and surgical intervention is required for definitive care. However, canine anaphylaxis must also be considered in all dogs with hemorrhagic effusions, some of which may have PT and aPTT times of <25% over the upper reference range, and thus not significantly coagulopathic (Lisciandro 2016b; Hnatusko et al. 2019). Because of this newly described complication in dogs, a focused spleen is now recommended following the AFAST examination in all canine hemoabdomens, and in general following any AFAST examinations in both dogs and cats (see Chapter 6and Figure 6.35. See also canine anaphylaxis and gallbladder wall edema section within this chapter).
The focused spleen is a rule‐in test, meaning that when a mass is detected, it is probably real (see Figure 6.35). In contrast, if a splenic mass is not seen then it could have been missed, depending on the proficiency of the sonographer and location of the mass. Thus, the focused spleen examination should be considered as it has high specificity as a screening test, but with variable sensitivity. The focused spleen is helpful because when a cavitated midabdominal mass is detected, especially when associated with the spleen and deforming its capsule, such a finding raises the probability of being correct in concluding that the hemoabdomen is due to a bleeding mass (surgical management) rather than canine anaphylaxis (medical management) (Lisciandro 2014a, 2016b). Any mass that deforms the capsule of the spleen should be considered a serious finding .
Pearl:In contrast to dogs, cats with spontaneous nontraumatic hemoabdomen have a poor prognosis because the cause is likely advanced forms of neoplasia (Mandell and Drobatz 1995; Culp et al. 2010). However, the AFAST‐applied AFS is helpful in predicting degree of anticipated anemia, the need for blood transfusion and exploratory laparotomy, or other hemostatic interventions. The Global FAST approach may also be used to stage the feline.
Major AFAST Difference Between Blunt and Penetrating Trauma
There is a major difference that must be understood when applying AFAST to blunt and penetrating trauma. The difference lies in the behavior of blood. In blunt trauma, it generally doesn't matter where the patient bleeds as mesothelial cells lining the abdominal cavity, pleural cavity, and pericardial sac rapidly defibrinate blood, making it readily apparent on AFAST as free fluid (anechoic triangulations). In contrast, victims of penetrating trauma have ripping, tearing and crushing of tissue, especially with bite wounds, and hence blood clots. During AFAST, clotted blood is often difficult to discriminate from adjacent soft tissue and thus is often initially missed ( Figure 7.6). Although there are no large veterinary studies (Lisciandro et al. 2008, 2009; Lisciandro 2012), the importance is likely similar to that in human medicine (Udobi et al. 2001), in that FAST is likely highly specific for surgical trauma but variably sensitive. AFAST (and Global FAST) should still be used as a first‐line screening test because of all the clinical questions that may be answered regarding the patient. However, in instances of a negative AFAST, serial examinations should be implemented as standard of care until it is clear whether the patient is surgical versus medical.
In time, clotted blood will defribinate and appear as free fluid, and when viscus organ injury is present, likely the organ will “leak” into the abdominal cavity. Thus, AFAST carries the potential to detect septic peritonitis and other developing complications earlier in their course. In fact, vascular injury, uroabdomen, bilioabdomen, gastrointestinal injury, and others may present over the next several days post injury. Parenchymal injury is also possible and the use of color flow Doppler can be helpful especially for screening for renal injury ( Figure 7.7). The author recommends continually performing AFAST serial examinations (or the Global FAST approach) four, eight, 12, and 24 hours post admission, and even two, three, and five days post injury. In other words, repeat the AFAST (Global FAST) as many times as needed until a surgical problem is comfortably ruled out.
Serial FAST examination strategies have proven helpful in human medicine (Blackbourne et al. 2004; Kirkpatrick et al. 2004; Ollerton et al. 2006; Matsushima and Frankel 2011; Mohammadi and Ghasemi‐Rad 2012). Although abdominal radiographs are of variable yield for blunt trauma because of their unreliability in detecting free fluid and their inability to semiquantitate volume (Lisciandro et al. 2009), radiography is always indicated in penetrating trauma as part of patient evaluation because of its ability to effectively detect hard tissue (fractures, luxations), soft tissue (herniation), and viscus organ injury (free air).
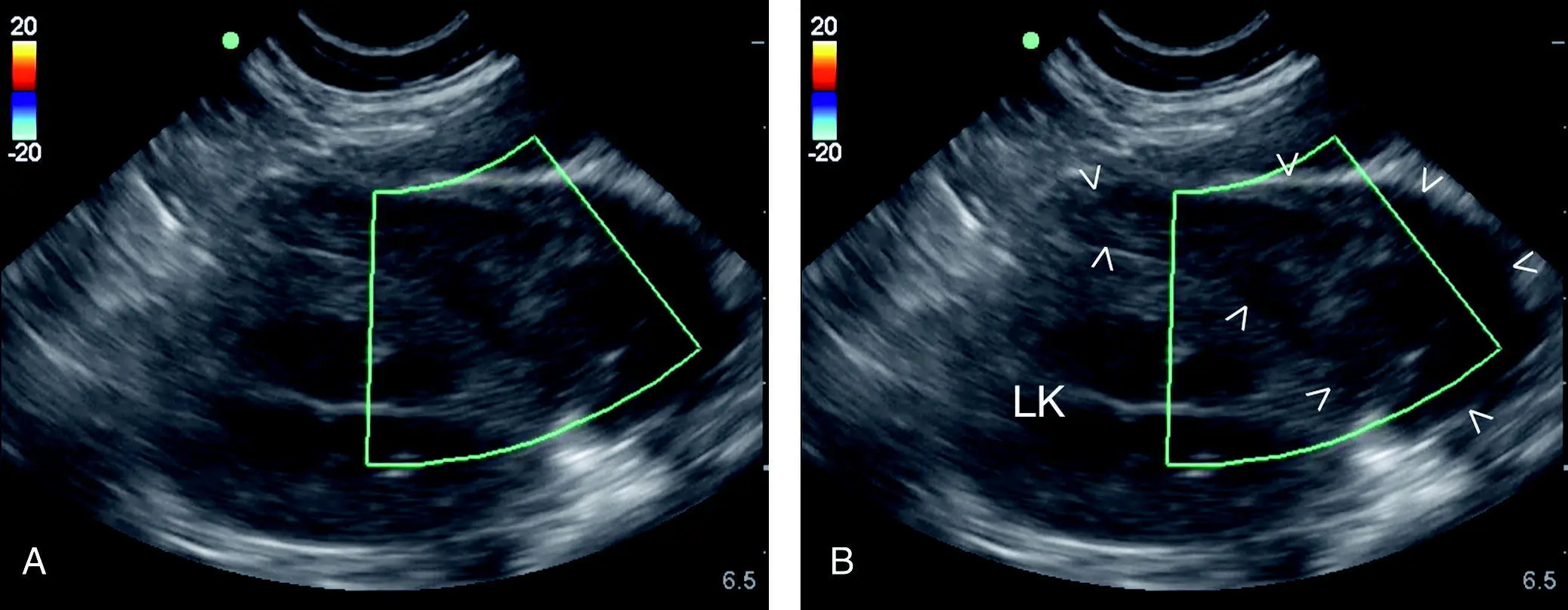
Figure 7.6. Clotted blood adjacent to the left kidney at the SR view. In penetrating trauma, blood often clots and clotted blood appears like soft tissue and is easy to miss during AFAST. Where suspected, color flow Doppler may be used. Clotted blood will lack flow. The image at the SR view shows the left kidney and an adjacent large clot with no flow on color Doppler, unlabeled in (A) and labeled in (B). Serial exams are key because if the clot was missed initially, the opportunity to capture the condition remains when repeating AFAST. Clot is outlined with cursors (V). LK, left kidney.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.