Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
| Type of trauma | Major injury/pathology, small‐volume bleeder(AFS 1, 2; modified AFS system <3) | Major injury/pathology, large‐volume bleeder(AFS 3, 4; modified AFS system ≥3) |
|---|---|---|
| Blunt trauma | ||
| Think Medical First Use AFS to help with decision‐making regarding transfusions and surgical intervention. Blood rapidly defibrinates thus is seen even acutely as anechoic (black) triangulations | If stays AFS 1, 2 (AFS <3) no blood transfusion necessary if only bleeding intraabdominallyDo NOT expect anemiaExpect PCV to be >30% in dogs and >24% in cats if only bleeding intraabdominallyIf stays AFS 1, 2 (AFS <3) and becomes anemic <30% in dogs and <24% in cats, rule out another site of bleeding (retroperitoneal, pleural cavity, fracture site, externally) so do Global FAST and a good physical examUncommon but possible for other nonhemorrhagic effusions (uroabdomen, bilioabdomen, other) | If an AFS 3, 4 (AFS ≥3) or becomes AFS ≥3 then expect anemia <30% in dogs and <24% in catsUse titrated fluid therapy strategies as 1/3 shock dose and repeat as fluid challenges are neededIf patient becomes severely anemic <25% in dogs and <20% in cats then generally treat medically first by blood transfusion(s)Note most intraabdominal bleeding in this subset will stop with 1 or 2 rounds of blood transfusion +/‐ replacement of clotting factorsUncommonly need exploratory surgeryUncommon but possible for other nonhemorrhagic effusions (uroabdomen, bilioabdomen, other) |
| Penetrating trauma | ||
| Think Surgical for Any Positive AFS Blood often acutely clots from ripping, tearing, crushing of tissue and thus is often missed during AFAST because clotted blood looks like adjacent soft tissue In time, blood clots will defibrinate and become free fluid, detected as anechoic (black) triangulations In time, ruptured, injured viscus organs will also leak or effuse, thus serial AFAST exams are key in cases in which medical vs surgical management is unclear Serial AFAST exams are key – at four, eight, 12 and 24 hours, two, three and five days You will miss a developing septic abdomen, pyothorax, by not using this strategy | Generally best to assume in penetrating trauma that all cases are surgical with ANY positiveCombine AFAST (or Global FAST) with other clinical findings and surgical indications (hernia, pneumoperitoneum, septic abdomen, refractory pain, etc.)Sample fluid when safely accessible and characterize the effusion with fluid analysis and cytologySerial exams are key – at four, eight, 12 and 24 hours, two, three and five daysYou will miss a developing septic abdomen, pyothorax, by not using this strategyCT is the gold standard imaging test | Generally best to assume in penetrating trauma that all cases are surgical with ANY positive, especially AFS 3 and 4Combine AFAST (or Global FAST) with other clinical findings and surgical indications (hernia, pneumoperitoneum, septic abdomen, refractory pain, etc.)Sample fluid when safely accessible and characterize the effusion with fluid analysis and cytologyCT is the gold standard imaging test |
| Postinterventional trauma | ||
| Think Medical for AFS 1, 2 and Surgical for AFS 3, 4 Large‐volume bleeding (AFS 3, 4) is generally not going to stop without surgical ligation of the bleeding Correct coagulopathy if present | If stays AFS 1, 2 (AFS <3) on serial exams, then generally NOT surgicalDo serial exams to make sure does not change score and become a large‐volume bleeder (AFS 3, 4)Sample fluid when safely accessible and characterize the effusion with fluid analysis and cytology | If an AFS 3, 4 and not anemic, then generally it is still best to explore emergently and NOT waitIf you wait, you will likely have to transfuse your patient with its added cost and more anesthetic riskIf an AFS 3, 4 and already anemic, transfuse as per patient assessment and explore emergentlySample fluid when safely accessible and characterize the effusion with fluid analysis and cytology |
Pearl:If an AFS 1, 2 (modified AFS system <3) “small‐volume bleeder” dog or cat without preexisting anemia becomes anemic, the attending clinician should explore other sites as potential sources of hemorrhage, including the retroperitoneal space, pericardial sac, pleural cavity, and lung, using the Global FAST approach along with a good physical exam.
Decision Making Using the AFS for the Hemoabdomen
Tables 7.2and 7.3will aid decision making based on the AFAST AFS score in dogs and cats.
In summary, the following general guidelines apply.
Blunt Trauma (BT)
Bleeding is most commonly medically treated with titrated fluid therapy, blood transfusion(s), and replacement of clotting factors in patients that require more than one transfusion or that are or have become coagulopathic. Surgery is uncommon so think medical treatment first .
Computed tomography (CT) is the gold standard for detecting injury, whereas AFAST provides indirect evidence through the detection of free fluid.
Radiography is an unreliable test for free fluid not only in terms of its presence or absence but also its inability to semiquantitate volume (Lisciandro et al. 2009).
Penetrating Trauma (PT)
Any positive is potentially a surgical problem and thus exploratory laparotomy should be considered post resuscitation. There are no veterinary studies evaluating positive AFAST studies and the frequency of medical versus surgical injuries; however, exploratory laparotomy is recommended in people with positive FAST examinations (Udobi et al. 2001).
Computed tomography is the gold standard for detecting injury, whereas AFAST provides only indirect evidence through the imaging of free fluid.
Other imaging options include radiography, which is standard of care for PT, for the detection of pneumoperitoneum, herniations, fractures and body wall abnormalities.
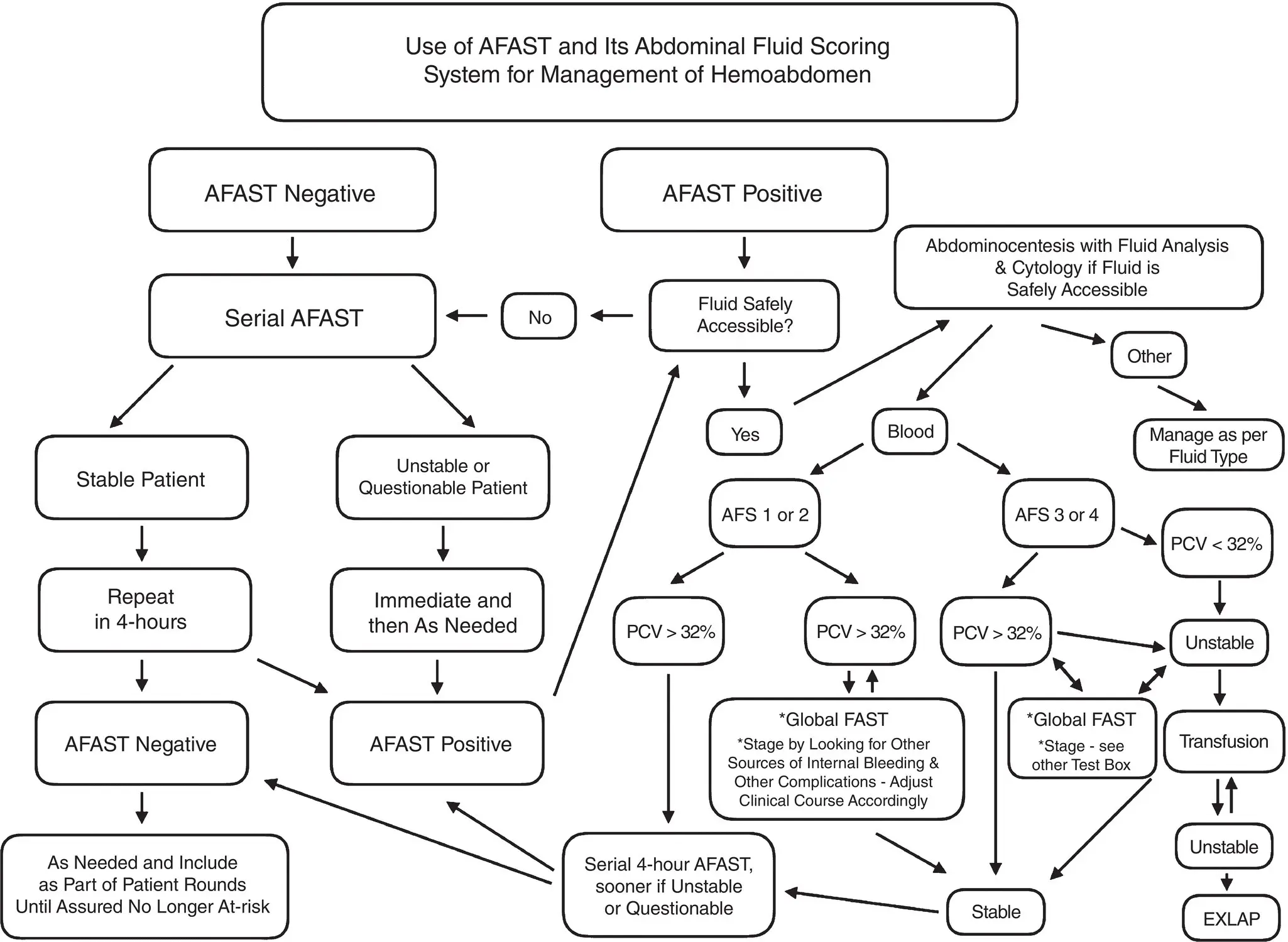
Table 7.3. Flowchart providing general guidelines regarding the decision‐making process for acutely bleeding dogs and cats when applying the abdominal fluid score (AFS) during AFAST. Note the algorithm assumes the patient is noncoagulopathic or, when coagulopathic, the coagulopathy is corrected.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Postinterventional Trauma
Apply the “small‐volume bleeder versus large‐volume bleeder” principle to determine if the case is medical or surgical. The postinterventional patient includes any invasive procedure in which internal bleeding is a possible complication, such as percutaneous aspirations, needle and Tru‐Cut biopsy, laparoscopy, exploratory laparotomy, etc.
Small‐Volume AFS 1 and 2 Bleeders
In general, the “small‐volume bleeder” (AFS 1 and 2; modified AFS system <3) is not immediately surgical and serial AFAST with an assigned AFS is an important monitoring tool for detecting increasing AFS often before overt decompensation, referred to as the “crump” (Bilello et al. 2011).
In stable AFS 1 and 2 (modified AFS system <3) patients, the author routinely repeats AFAST with an assigned AFS ~1 hour post admission and then again four hours post admission, and then as clinical course dictates.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.