Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Isoechoic (same echogenicity): occurs when tissues are the same shades of gray. For example, if the liver is isoechoic to the spleen then they are the same echogenicity (same shades of gray).
How Ultrasound Behaves Relative to Tissues and Elements
The knowledge of how ultrasound behaves relative to the structures and elements it encounters is very important. From normal tissues within the body to its various constituents (elements) of fluid, air, and mineralization, ultrasound behaves differently, causing a number of artifacts, which can be learned with diligent study, training, and practice. Foreign materials, such as plastic, metal, bone, stone, glass, and vegetative materials, also cause predictable artifacts. These artifacts will be covered in the next few chapters and throughout the textbook. It is a good idea to consider them every time you look at an image to accelerate your learning process.
Degrees of echogenicity of commonly encountered structures from hypoechoic to hyperechoic structures are listed in Table 1.1.
Ultrasound Screen Orientation
The screen orientation should always be “head to the left and tail to the right,” similar to the orientation for radiography ( Figure 1.6). Thinking in this manner will help you learn the anatomy you are seeing and help you with the direction you need to go to get to the POCUS and FAST ultrasound structures of interest. The exception to this rule is that most cardiologists reverse the screen orientation of the heart, which is very problematic for learning image acquisition when doing a Global FAST approach. Many human institutions have rejected this approach for the noncardiologists performing POCUS and FAST examinations for the aforementioned reason.
Table 1.1. Degrees of echogenicity of commonly encountered structures.
| Structure | |
|---|---|
| Anechoic – hypoechoic (black) | Bile, urine |
| Darker Shades of grayBrighter | Muscle |
| Renal medulla | |
| Renal cortex | |
| Liver | |
| Fat | |
| Spleen | |
| Prostate | |
| Renal sinus | |
| Vessel walls | |
| Hyperechoic (white) | Bone, air, gas |
Directional Terms for Orientation
Longitudinal and Sagittal
The term longitudinal refers to orientation parallel to the spine or long axis of the patient’s body (see Figures 4.1, 4.2, 4.3). The term sagittal refers to the longitudinal axis of the respective deeper structure being evaluated. For example, the superficial jugular vein is imaged in longitudinal whereas the more deeply located and oblique right kidney (not parallel to the body’s long axis) is imaged in sagittal planes (parallel to the right kidney’s long axis). The terms are often used interchangeably (or, arguably, misused); however, by appreciating that both terms are in their own right long‐axis views, directional communication between veterinarians seems to be clear by use of either term. Thus in longitudinal planes, the probe marker is directed towards the patient's head to maintain the same orientation as radiography, head to the left and tail to the right of ultrasound (and radiographic) image.
Transverse
The term transverse refers to orientation 90° to the long axis of the structure being evaluated or the short axis of the patient (see Figures 4.1, 4.2, 4.3). The probe marker is turned to the left (or counterclockwise) to the patient’s right side. Thus, in transverse planes, the probe marker is directed to the patient's right side to maintain the same orientation as radiography, right side on left side of ultrasound (and radiographic) image.
With that said, let’s get on with Dr Fulton’s chapters that will cover in more detail the physics of ultrasound, its artifacts, and various pointers on the ultrasound machine features and settings and image acquisition.
It's worth your effort and time investment to learn this core skill – POCUS and FAST improve care and save lives!
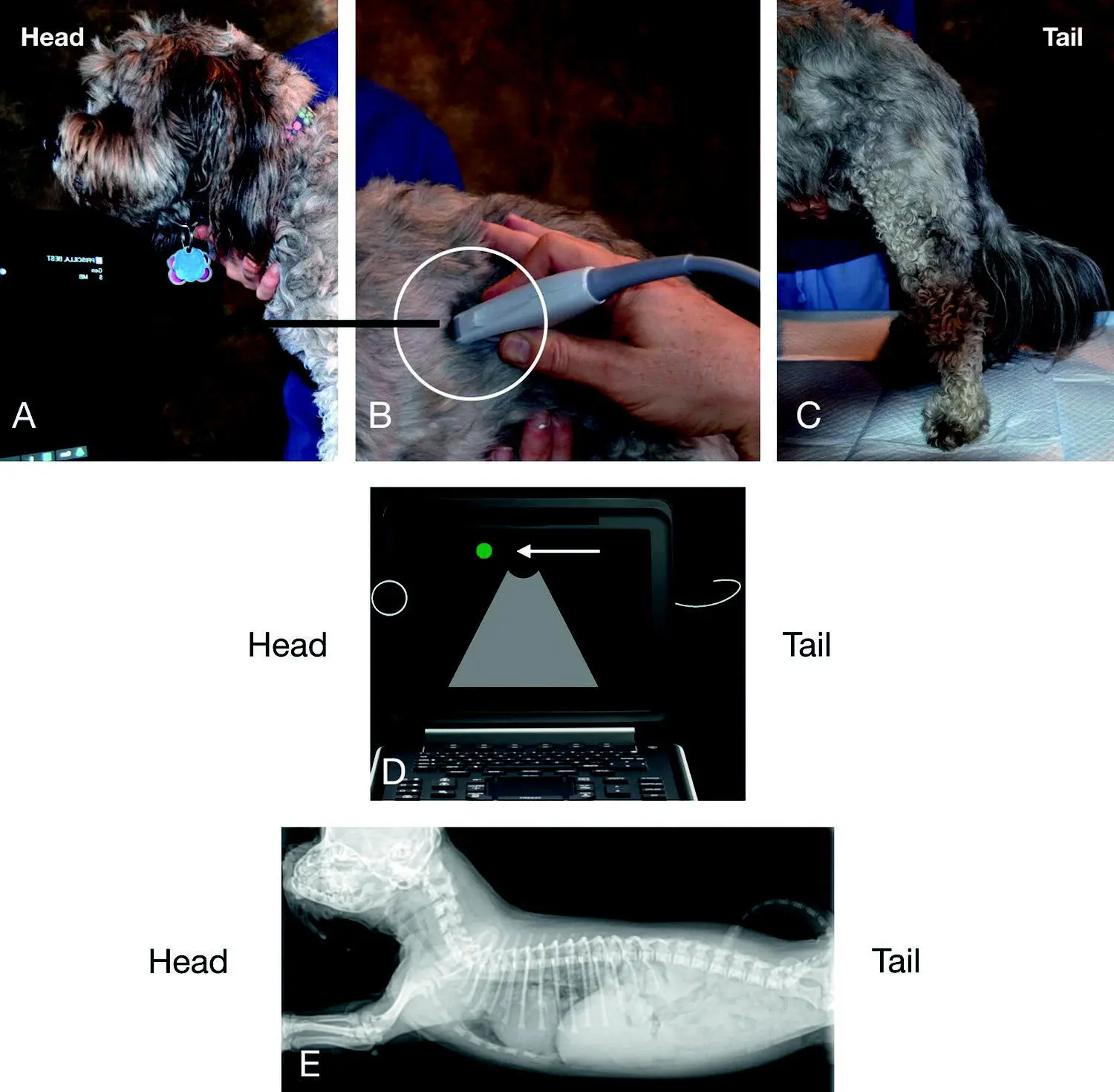
Figure 1.6. Longitudinal (sagittal) planes and orientation. Make the screen marker and the probe marker both consistent with “head to the left and tail to the right,” which is the same orientation as radiography. (A) shows the head of the dog and (C) its tail. In (B), the probe is placed on the truncal area of the same dog. The white circle highlights the probe marker (can be a notch, a raised line or button, or an LED light). Every probe has its marker. In (D) is a pictorial of the ultrasound screen, and the green dot indicates the screen marker (arrow ←). Make sure that this is to the left of the screen and the probe marker is toward the head of your patient. In (E) is a radiograph showing the same orientation used for ultrasound, “head to the left, tail to the right.” Courtesy of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
References
1 Kirkpatrick AW, Sirois M, Laupland KB, et al. 2004. Hand‐held thoracic sonography for detecting post‐traumatic pneumothoraces: the extended focused assessment with sonography for trauma (EFAST). J Trauma 57:288–295.
2 Lisciandro GR. 2011. Abdominal and thoracic focused assessment with sonography for trauma, triage, and monitoring in small animals. J Vet Emerg Crit Care 21(2):104–122.
3 Lisciandro GR. 2016. The use of the diaphragmatico‐hepatic (DH) views of the abdominal and thoracic focused assessment with sonography for triage (AFAST/TFAST) examinations for the detection of pericardial effusion in 24 dogs (2011–2012). J Vet Emerg Crit Care 26(1):125–131.
4 Lisciandro GR, Lagutchik MS, Mann KA, et al. 2008. Evaluation of a thoracic focused assessment with sonography for trauma (TFAST) protocol to detect pneumothorax and concurrent thoracic injury in 145 traumatized dogs. J Vet Emerg Crit Care 18(3):258–269.
5 Lisciandro GR, Lagutchik MS, Mann KA, et al. 2009. Evaluation of an abdominal fluid scoring system determined using abdominal focused assessment with sonography for trauma in 101 dogs with motor vehicle trauma. J Vet Emerg Crit Care 19(5):426–437.
6 Lisciandro GR, Fosgate GT, Fulton RM. 2014. Frequency of ultrasound lung rockets using a regionally‐based lung ultrasound examination named veterinary bedside lung ultrasound exam (Vet BLUE) in 98 dogs with normal thoracic radiographic lung findings. Vet Rad Ultrasound 55(3):315–322.
7 Lisciandro GR, Fulton RM, Fosgate GT, Mann KA. 2017. Frequency of B‐lines using a regionally‐based lung ultrasound examination (the Vet BLUE protocol) in 49 cats with normal thoracic radiographical lung findings. J Vet Emerg Crit Care 27(3):267–277.
8 McMurray J, Boysen S, Chalhoub S. 2016. Focused assessment with sonography in nontruamtized dogs and cats in the emegrency and critivcal care setting. J Vet Emerg Crit Care 26(1):64–73.
9 Rozycki GS. 1998. Surgeon performed US: its use in clinical practice. Ann Surg 228:16–28.
10 Rozycki GS, Ballard RB, Feliciano DV, et al. 1998. Surgeon‐performed ultrasound for the assessment of truncal injuries: lessons learned from 1540 patients. Ann Surg 228(4):557–567.
11 Rozycki GS, Pennington SD, Feliciano DV. 2001. Surgeon‐performed ultrasound in the critical care setting: its use as an extension of the physical examination to detect pleural effusion. J Trauma 50(4):636–642.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.