James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
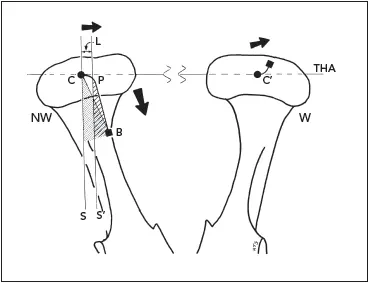
Fig 2-9In the nonworking condyle (NW), the traditional Bennett angle (SCB) measures the angle from the sagittal plane to the endpoint of the movement of the condyle center. The Bennett angle used in articulators with an immediate lateral translation capability (S’PB) is measured from the sagittal plane after the immediate or early lateral translation (L) has occurred. The transverse horizontal axis (THA), or hinge axis of purely rotational movement, extends through both condyles. The working side condyle (W) slides laterally, or outward, in laterotrusion.
The bodily shift of the mandible in the direction of the working side was first described by Bennett. 14The angle formed in the horizontal plane between the pathway of the nonworking condyle, the mandibular lateral translation, and the sagittal plane is called the Bennett angle ( Fig 2-9). The presence of an immediate or early lateral translation, or side shift, has been reported in 86% of the condyles studied. 15In addition to confirming the predominant presence of the early lateral translation, Lundeen and Wirth, using a mechanical apparatus, showed its median dimension to be approximately 1.0 mm with a maximum of 3.0 mm. 16Hobo and Mochizuki, using an electronic measuring device, found a lower mean value of 0.4 mm for the immediate lateral translation, with a high of 2.6 mm. 17,18
Following the immediate lateral translation, there is a further gradual shifting of the mandible, or progressive lateral translation, which occurs at a rate proportional to the forward movement of the nonworking condyle. 19At one time, this was known as progressive side shift or Bennett side shift . Lundeen and Wirth found slight variation in the direction of the progressive lateral translation or Bennett angle, with a mean value of 7.5 degrees. 16Hobo and Mochizuki found a much greater variation, ranging from 1.5 to 36 degrees, with a mean value of 12.8 degrees. 17,18
Determinants of mandibular movement
The two condyles and the contacting teeth are analogous to the three legs of an inverted tripod suspended from the cranium. The determinants of the movements of that tripod are, posteriorly, the right and left TMJs; anteriorly, the teeth of the maxillary and mandibular arches; and overall, the neuromuscular system. 20
The dentist has no control over the posterior determinants, the TMJs; they are unchangeable. However, they influence the movements of the mandible, and of the teeth, by the paths that the condyles must travel when the mandible is moved by the muscles of mastication. The measurement and reproduction of those condylar movements is the basis for the use of articulators.
The anterior determinant, the teeth, provides guidance to the mandible in several ways. The posterior teeth provide the vertical stops for mandibular closure. They also guide the mandible into the position of maximal intercuspation, which may or may not correspond with the optimum position of the condyles in the glenoid fossae. The anterior teeth (canine to canine) help to guide the mandible in right and left lateral excursive movements and in protrusive movements. Anterior teeth are especially suited for guidance by virtue of:
Canines having the longest, strongest roots in their respective arches
The load being reduced by distance from the fulcrum (Class III lever)
The proprioceptive threshold and concomitant reflexes reducing the load 21– 23
Dentists have direct control over the tooth determinant by orthodontic movement of teeth; restoration of the anterior lingual or posterior occlusal surfaces; and equilibration, or selective grinding, of any teeth that are not in a harmonious relationship. Intercuspal position and anterior guidance can be altered, for better or for worse, by any of these means.
The closer a tooth is located to a determinant, the more it will be influenced by that determinant ( Fig 2-10). A tooth located near the anterior region will be influenced greatly by anterior guidance and less by the TMJ. A tooth in the posterior region will be influenced partially by the joints and partially by anterior guidance.
The neuromuscular system, through proprioceptive nerve endings in the periodontium, muscles, and joints, monitors the position of the mandible and its paths of movement. Through reflex action, it will program the most physiologic paths of movement possible under the set of circumstances present. Dentists have indirect control over this determinant through procedures performed on the teeth, which may affect the response of the neuromuscular system.
One of the objectives of restorative dentistry is to place the teeth in harmony with the TMJs. This results in minimum stress on the teeth and joints, with only a minimum effort expended by the neuromuscular system to produce mandibular movements. When the teeth are not in harmony with the joints and the movements of the mandible, an interference is said to exist.
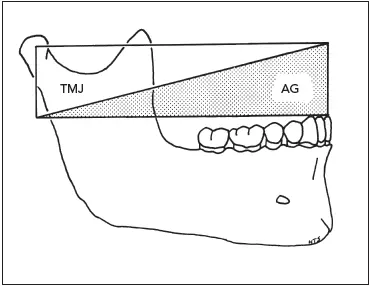
Fig 2-10The farther anterior a tooth is located, the less the influence of the TMJ and the greater the influence of the anterior guidance (AG).
Occlusal interferences
Interferences are undesirable occlusal contacts that may produce mandibular deviation during closure to maximal intercuspation or may hinder smooth passage to and from the intercuspal position. There are four types of occlusal interferences:
1 Centric
2 Working
3 Nonworking
4 Protrusive
The centric interference is a premature contact that occurs when the mandible closes with the condyles in their optimum position in the glenoid fossae ( Fig 2-11). It will cause deflection of the mandible in a posterior, anterior, and/or lateral direction. 24
A working interference may occur when there is contact between the maxillary and mandibular posterior teeth on the same side of the arches as the direction in which the mandible has moved ( Fig 2-12). If that contact is heavy enough to disocclude anterior teeth, it is an interference. 25
A nonworking interference is an occlusal contact between maxillary and mandibular teeth on the side of the arches opposite the direction in which the mandible has moved in a lateral excursion ( Fig 2-13). The nonworking interference is particularly destructive in nature. 26–29The potential for damaging the masticatory apparatus has been attributed to changes in the mandibular leverage, the placement of forces outside the long axes of the teeth, and disruption of normal muscle function. 30
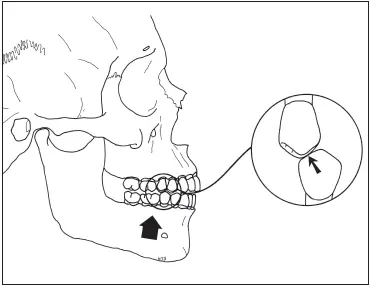
Fig 2-11A centric occlusal interference often occurs during mandibular closure between maxillary mesial-facing cusp inclines and mandibular distal-facing inclines. As a result, the mandible is deflected anteriorly.
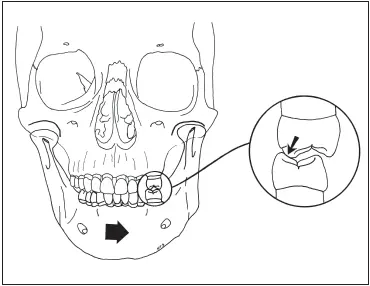
Fig 2-12A working interference may occur between maxillary palatal-facing cusp inclines and mandibular facial-facing cusp inclines on the working side.
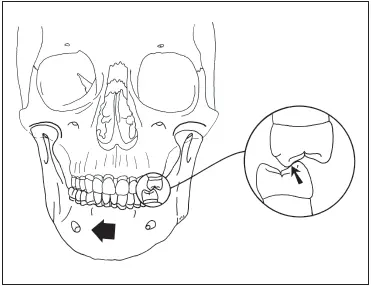
Fig 2-13A nonworking interference results when there is contact between maxillary facial-facing cusp inclines and mandibular lingualfacing cusp inclines on the nonworking side.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.