James C. Kessler - Fundamentals of Fixed Prosthodontics
Здесь есть возможность читать онлайн «James C. Kessler - Fundamentals of Fixed Prosthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Fixed Prosthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Fixed Prosthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Fixed Prosthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Fixed Prosthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Fixed Prosthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
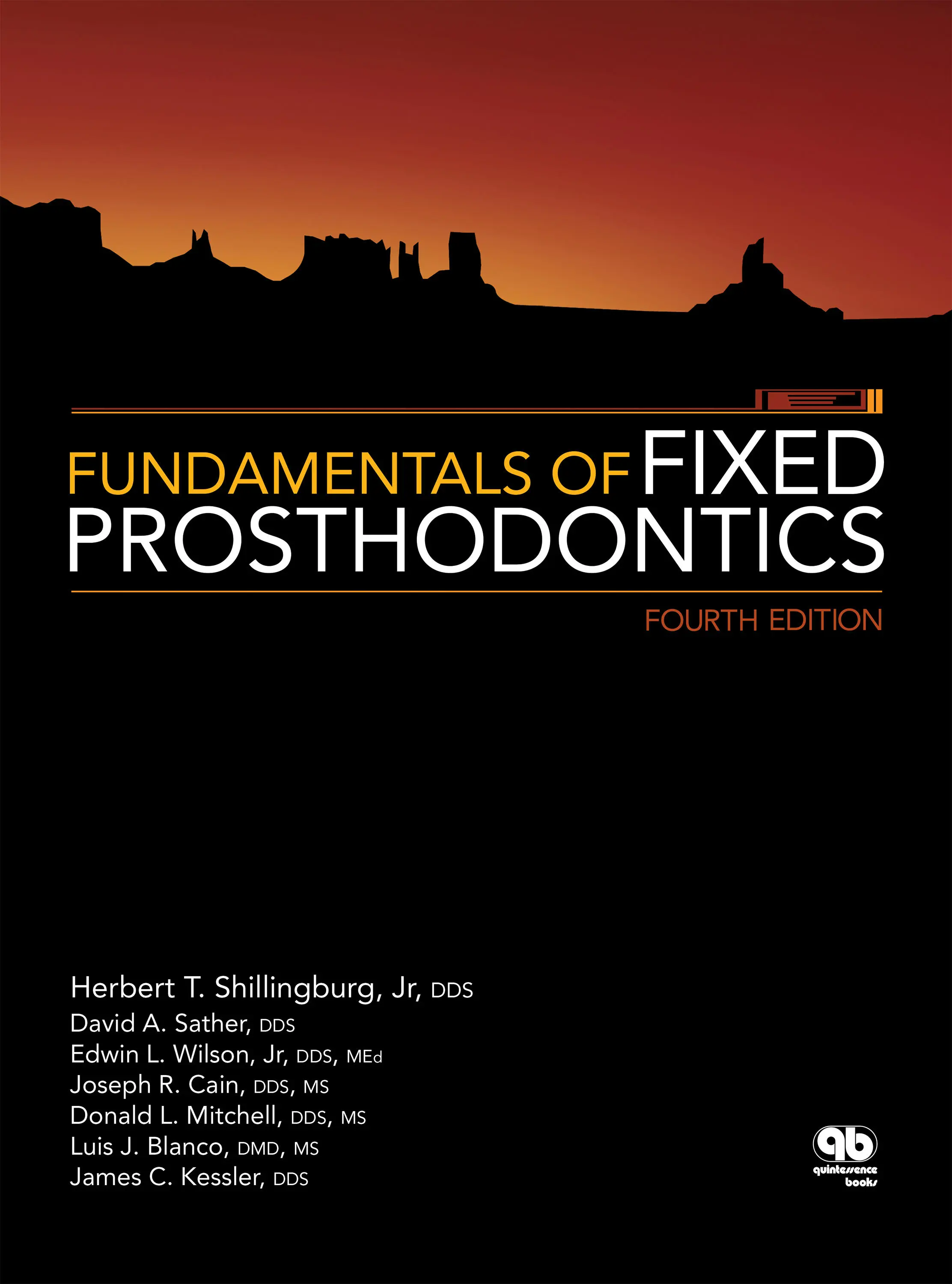
The articular disc is biconcave, devoid of nerves and blood vessels in the central area, and tough—much like a piece of shoe leather. It has a few muscle fibers attached in the anterior aspect from the superior lateral pterygoid muscle. The disc is attached to the condyle on its medial and lateral aspects and should be interposed between the condyle and articular eminence during function. The condyle is not spherical but has an irregular, elliptical shape. This shape helps to distribute stress throughout the TMJ rather than concentrating it in a small area.
Many methods have been used to guide the mandible into an optimal position. Earlier concepts of centric relation involved the most posterior condylar position in the fossa. The condyle was sometimes forcefully manipulated into the rearmost, uppermost, and midmost (RUM) position within the glenoid fossa, 4,6–8using chin point guidance. However, when the condyle is retruded, it might not be seated on the central area of the articular disc; instead, it might be on the highly vascular and innervated retrodiscal tissues (the posterior attachment) posterior to the disc 9( Fig 2-2). This can occur if the inner horizontal portion of the temporomandibular ligament has been unduly traumatized so that it no longer supports the condyle in a more anterior, physiologic position. It is presently thought that rather than being a physiologic position, this is frequently an abnormal, forced position that could create unnecessary strain in the TMJ. In this circumstance, the disc is displaced anteriorly, and clicking of the joint is frequently observed as the patient opens and closes.
The more recent concept describes a physiologic position in terms of the musculoskeletal relationships of the structures 10( Fig 2-3). It is not a forced position; rather, the mandible is gently guided by the operator using the bilateral method 11or by allowing natural muscle action to place the condyle in a physiologically unstrained position. 12
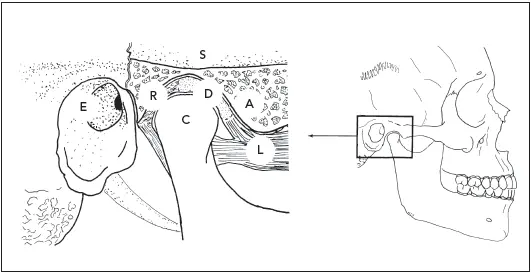
Fig 2-1Some of the components of the TMJ. A, articular eminence; C, condyle; D, articular disc; E, external auditory meatus; L, superior and inferior lateral pterygoid muscles; R, retrodiscal tissue (posterior attachment); S, thin superior wall of the glenoid fossa.
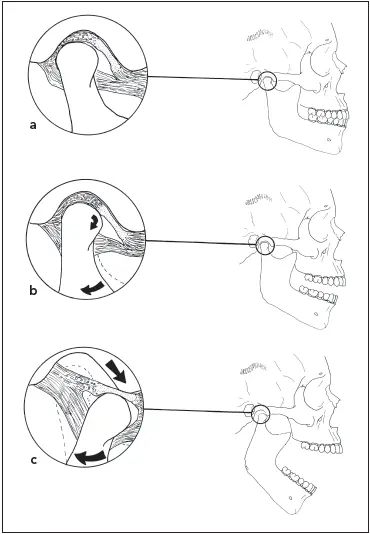
Fig 2-2 (a) In a dysfunctional joint with an internal derangement, the disc is displaced anterior to the condyle at the intercuspal position. (b) After initial rotational opening, the condyle is still posterior to the disc. (c) In translation of the mandible to maximum opening, the condyle recaptures the disc, clicking into position as it does.
Fig 2-3(a) In a healthy joint, the condyle is in a superoanterior position in the fossa with the articular disc interposed when the teeth are in maximal intercuspation. (b) In the initial stage of opening, the condyle rotates in position, with the disc remaining stationary. (c) In maximum opening, the condyle translates forward, with the disc still interposed.
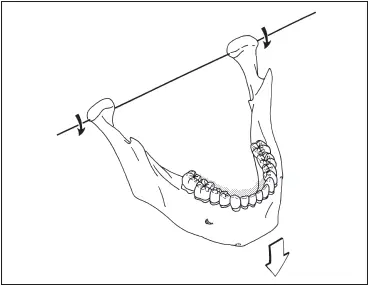
Fig 2-4The mandible moves on a horizontal axis, as seen in a hinge axis opening.
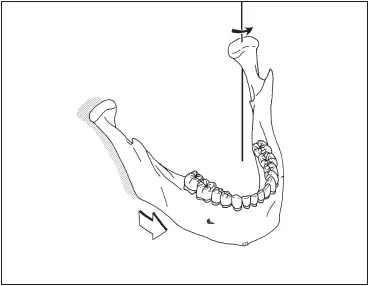
Fig 2-5Mandibular movement occurs around a vertical axis during a lateral excursion.
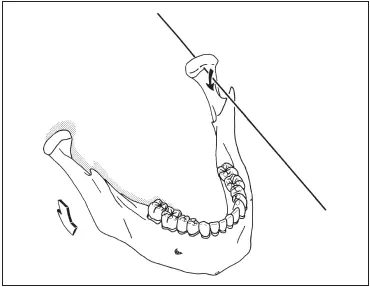
Fig 2-6The mandible also rotates around a sagittal axis when one side drops down during a lateral excursion.
Mandibular Movement
Mandibular movement can be broken down into a series of motions that occur around three axes:
1 Horizontal axis ( Fig 2-4): This movement, in the sagittal plane, happens when the mandible in centric relation makes a purely rotational opening and closing border movement around the transverse horizontal axis, which extends through both condyles.
2 Vertical axis ( Fig 2-5): This movement occurs in the horizontal plane when the mandible moves into a lateral excursion. The center for this rotation is a vertical axis extending through the rotating or working-side condyle.
3 Sagittal axis ( Fig 2-6): When the mandible moves to one side, the condyle on the side opposite the direction of movement travels forward. As it does, it encounters the eminence of the glenoid fossa and moves downward simultaneously. When viewed in the frontal plane, this produces a downward arc on the side opposite the direction of movement, rotating around an anteroposterior (sagittal) axis passing through the other condyle.
Various mandibular movements are composed of motions occurring concurrently around one or more of the axes. The up-and-down motion of the mandible is a combination of two movements. A purely hinge movement occurs as the result of the condyles rotating in the lower compartments of the TMJs within a 10- to 13-degree arc, which creates a 20- to 25-mm separation of the anterior teeth (see Fig 2-3b). This phenomenon was the basis for the terminal hinge axis theory in the early 1920s by McCollum. 3Kohno verified the presence of a transverse horizontal axis, which he termed the kinematic axis. 13There is also some gliding movement in the upper compartment of the joint if the mandible drops down farther (see Fig 2-3c). Then the axis of rotation shifts to the area of the mandibular foramen, as the condyles translate forward and downward while continuing to rotate.
When the mandible slides forward so that the maxillary and mandibular anterior teeth are in an end-to-end relationship, it is in a protrusive position. Ideally, the anterior segment of the mandible will travel a path guided by contacts between the anterior teeth, with complete disocclusion of the posterior teeth ( Fig 2-7).
Mandibular movement to one side will place it in a working, or laterotrusive, relationship on that side and a nonworking, or mediotrusive, relationship on the opposite side; eg, if the mandible is moved to the left, the left side is the working side and the right side the nonworking side ( Fig 2-8). In this type of movement, the condyle on the nonworking side will arc forward and medially (see A in Fig 2-8). Meanwhile, the condyle on the working side will shift laterally and usually slightly posteriorly (see B in Fig 2-8).
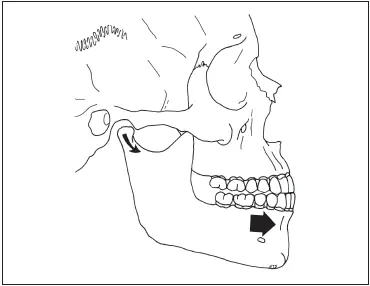
Fig 2-7A protrusive movement occurs when the mandible moves forward.
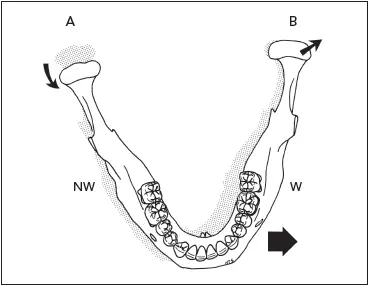
Fig 2-8When the mandible moves into a left lateral excursion, the right condyle (A) moves forward and inward, while the left condyle (B) will shift slightly in a lateroposterior direction. In this example, the left side is the working side (W), and the right side is the nonworking side (NW).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Fixed Prosthodontics»
Представляем Вашему вниманию похожие книги на «Fundamentals of Fixed Prosthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Fixed Prosthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.