Katherine Kula - Cephalometry in Orthodontics
Здесь есть возможность читать онлайн «Katherine Kula - Cephalometry in Orthodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Cephalometry in Orthodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Cephalometry in Orthodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Cephalometry in Orthodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Cephalometry in Orthodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Cephalometry in Orthodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
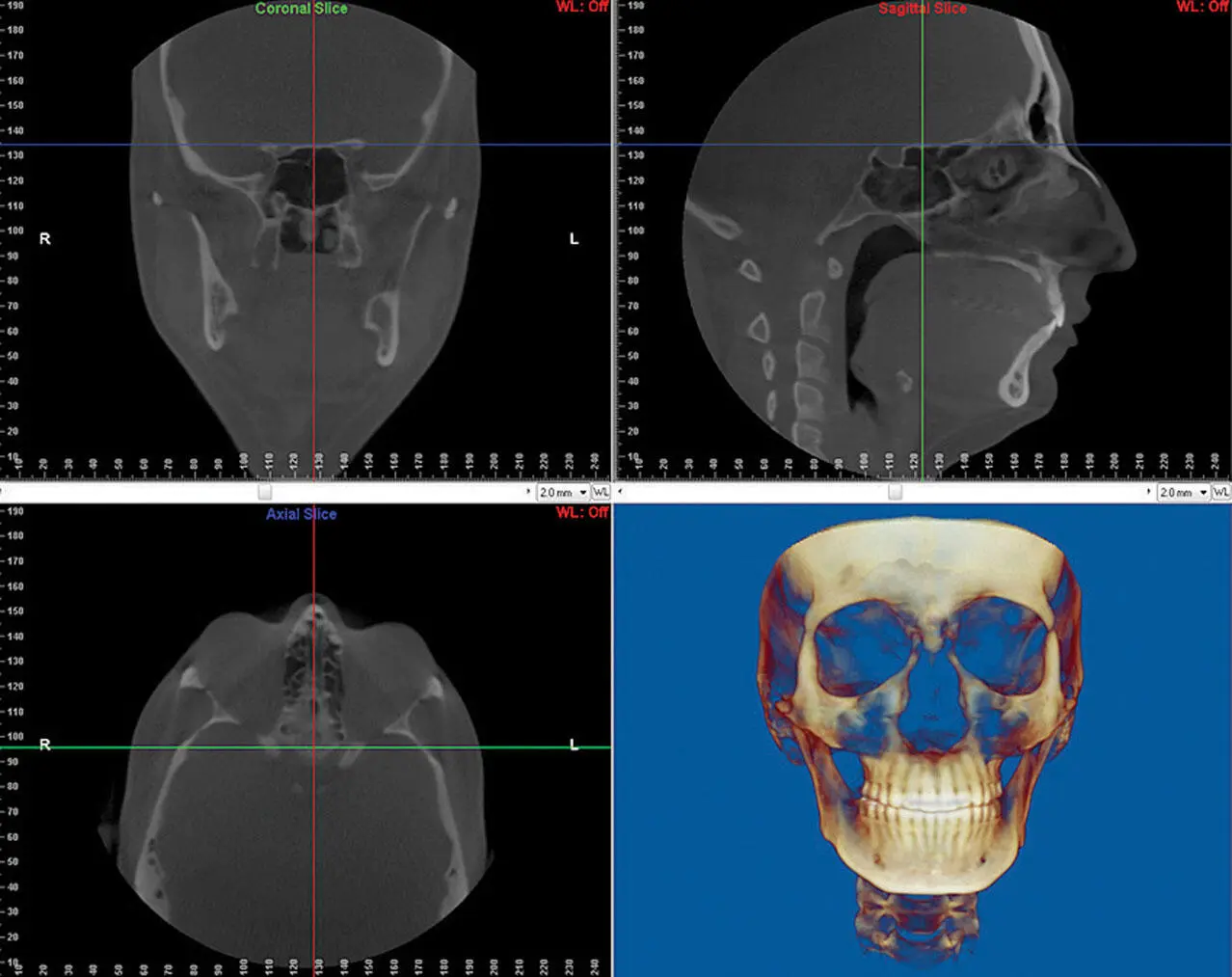
Fig 1-2Software screen showing (a) coronal slice ( green line in b and c ), (b) sagittal slice ( red line in a and c ), (c) axial slice ( blue line in a and b ), and (d) 3D CBCT reconstruction of the same study.
The general purpose of this book is to introduce the orthodontic clinician to the use and interpretation of cephalometrics, both 2D and 3D, and to show the potential benefits of using 3D CBCTs. The purpose of this chapter is to provide the background for the current and future use of cephalometrics.
History of Cephalometrics
Prior to the use of radiographs, growth and development of the craniofacial complex was essentially a study of skull measurements (craniometry) ( Fig 1-3) or soft tissue. Craniometry 2dates back to Hippocrates in the 4th century BC and is still used today in physical anthropology, forensics, medicine, and art. It is used to determine the size of cranial bones and teeth, their relationship to each other, potential differences among groups of people, and evolutionary changes in the cranium and face. Some of the current cephalometric landmarks, planes, and angles have their origin in craniometry. For example, the Frankfort plane was established in 1882 during a meeting of the German Anthropological Society as a standardized method of orienting the skull horizontally for measurements. 2The anthropologists agreed to define the Frankfort plane as a plane from the upper borders of the auditory meati (external auditory canals) to the inferior margins of each orbit. Later, this plane was modified for cephalometry to indicate that the right and left porion and left orbitale would be used to define the horizontal plane to minimize problems that asymmetry caused.
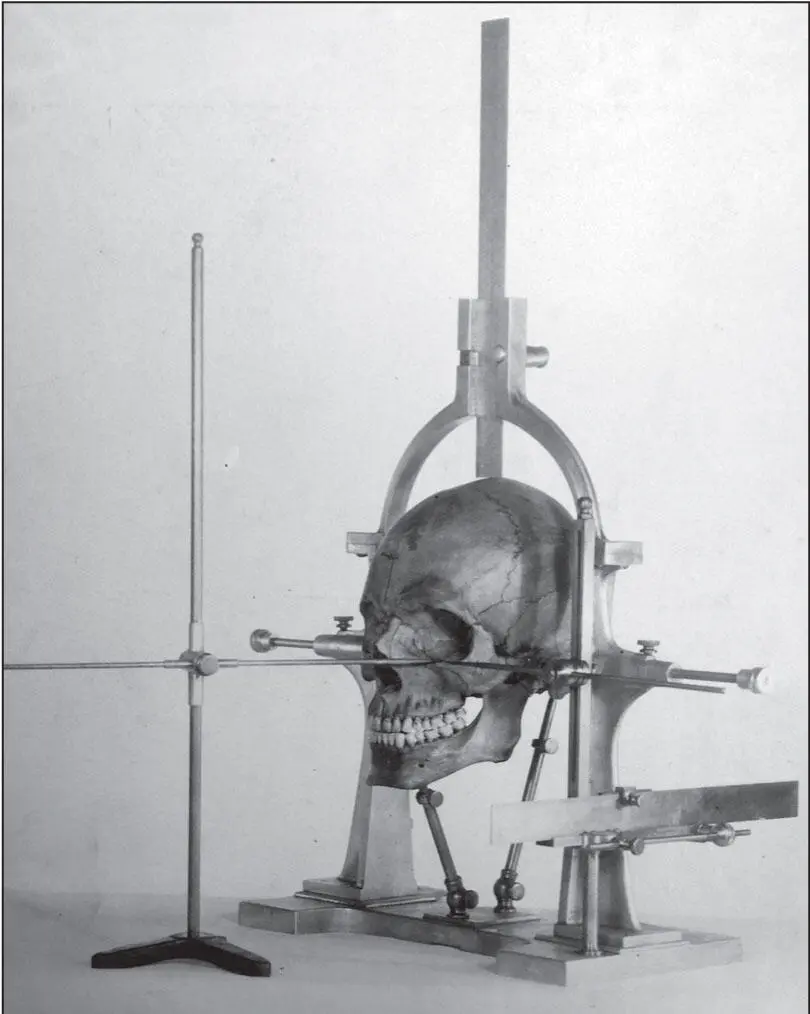
Fig 1-3An original Broadbent craniostat used to standardize skull position and measurement. (Courtesy of Dr Juan Martin Palomo, Case Western Reserve University.)
Craniometry, however, had limitations. Each skull represented a one-time peek or snapshot at the development of one individual—in other words, a cross-sectional data point. There was little hope of a longitudinal study. Frequently, the reason for the death of the individual was unknown, resulting in an unknown effect on the growth and development of the skull. Thus, craniofacial development was interpreted based on the skulls of children who died because of trauma, disease, starvation, abuse, or genetics. Todd, 3the chairman of the Department of Anatomy at Case Western Reserve University School of Medicine, considered the measuring of these children’s skulls as studying defective growth and development; the longitudinal effect of orthodontic treatment on growth and development could not be assessed. Animal studies using dyes were obviously limited in providing interpretation of the effect of various factors on human growth and development. Soft tissue studies, particularly longitudinal, were also limited by the lack of reproducible data. Radiographs, however, provided the opportunity to study and compare multiple patients over decades.
The use and standardization of cephalograms continually evolved from their early beginnings in the late 1800s. Similarly, during that time, orthodontics had its inception as a dental specialty. Edward Hartley Angle classified malocclusion in 1899 and was recognized by the American Dental Association for making orthodontics a dental specialty. 4Angle established the first school of orthodontics (Angle School of Orthodontia in St Louis) in 1900, the first orthodontic society (American Society of Orthodontia) in 1901, and the first dental specialty journal (American Orthodontist) in 1907.
Shortly after the discovery of x-rays by Wilhelm Conrad Roentgen in 1895, 5the use of the first facial and cranial radiographs was reported as early as 1896 by Rowland 6and later by Ketcham and Ellis. 7By 1921, B. H. Broadbent was using lateral cephalograms in his private practice. 7In 1922, Spencer Atkinson reported to the Angle College of Orthodontia that he used lateral facial radiographs to identify the position of the first molar below the maxilla’s key ridge. 7Because the radiographs also showed soft tissue, Atkinson suggested that these lateral radiographs had the potential of relating the mandible and the maxilla to the face and to the cranial base.
Initially, the comparison of cephalometric radiographs to show the effects of growth and treatment was difficult because head position and distance from the cephalometric film were not standardized. In an attempt to standardize head position, in 1921 Percy Brown designed a head holder for taking radiographic images of the face. 7In 1922, A. J. Pacini reported standardizing head position for lateral radiographs by using a gauze bandage to hold the film to the head. 8Ralph Waldron followed in 1927 by constructing a cephalometer to measure the gonial angle on a roentgenogram taken 90 degrees from the profile. 9Martin Dewey and Sidney Riesner held the patient’s head in a clamp and took a profile view with the film cassette placed against the head. 10However, for several decades there was no universal standardization of cephalometric technique, meaning that identical radiographs of the same patient could not be reproduced.
It was obvious to Broadbent 11that accurate and reliable longitudinal measurements of the head and face in three dimensions would be necessary to study growth and development of the teeth and the jaws as well as the effect of orthodontic treatment. Drawing on his previous experience of modifying Todd’s craniostat into a craniometer to standardize skull position and measurement (see Fig 1-3), Broadbent developed a craniostat that consisted of a head-holding device, two ear rods, and a nasion rest to stabilize the head of a living person relative to the radiographic film and the x-ray source ( Fig 1-4). Broadbent even took impressions of the teeth while the patient was positioned in the craniostat and related them to the maxilla and mandible. He announced in 1930 that he had used a radiographic craniostat to study the longitudinal growth of the living face 12and published a description of the invention in 1931. 11Bolton’s cephalostat was modified later to include the standardization of head position for a roentgenogram from the frontal view ( Fig 1-5). During the same year, a German orthodontist, H. Hofrath, also reported the development of a craniostat to standardize head position while taking lateral radiographs. 13
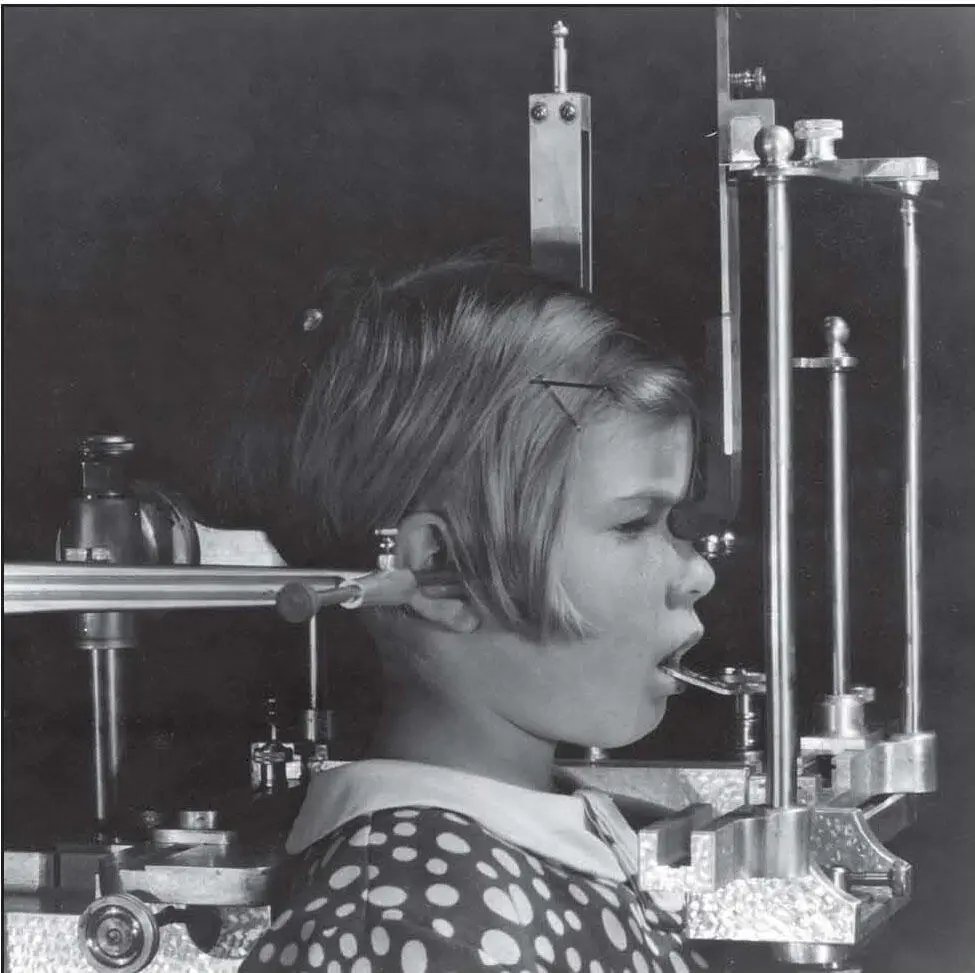
Fig 1-4An original Broadbent cephalometric craniostat consisting of a head-holding device, two ear rods, and a nasion rest to stabilize the head of a living person relative to the radiographic film and the x-ray source. (Courtesy of Dr Juan Martin Palomo, Case Western Reserve University.)
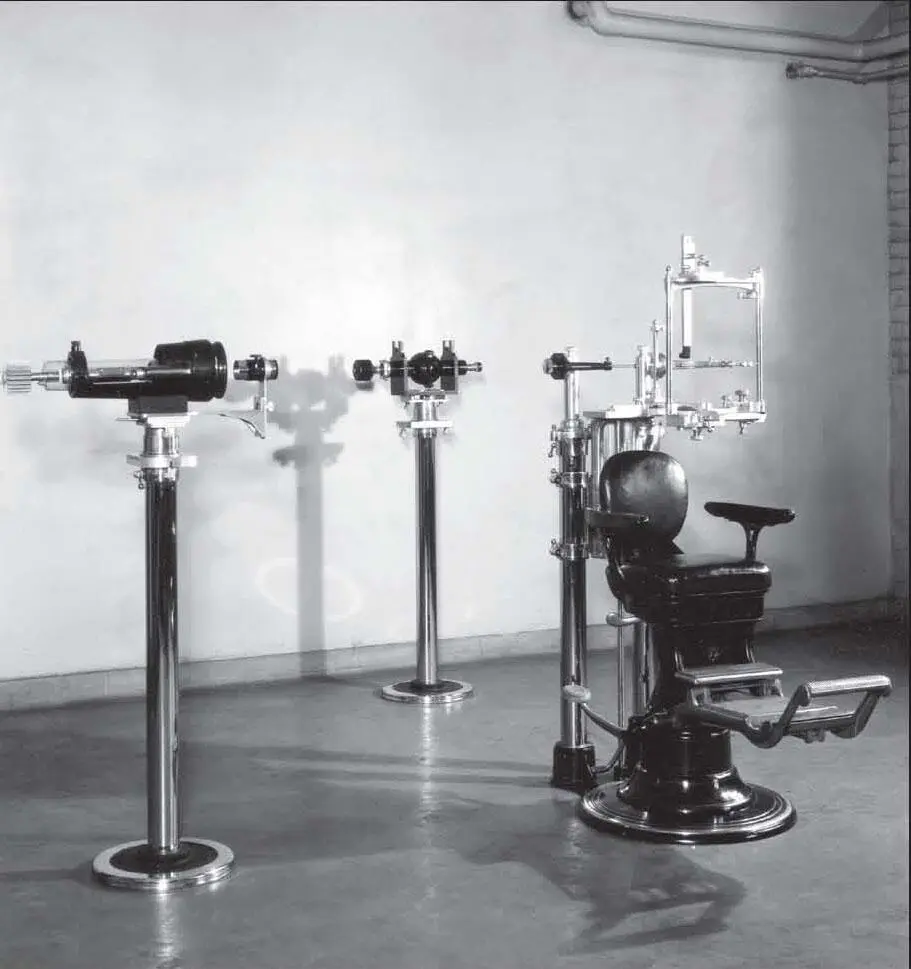
Fig 1-5An original Bolton cephalostat modified to standardize head position for a frontal roentgenogram. (Courtesy of Dr Juan Martin Palomo, Case Western Reserve University.)
The standardization of cephalograms allowed comparison of the same head over time. Treatment effects and comparison with other individuals could also be studied. This so impressed Congresswoman Frances Bolton that she established a long-term research study at Case Western Reserve University to examine the growth and development of the teeth and the jaws in healthy children.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Cephalometry in Orthodontics»
Представляем Вашему вниманию похожие книги на «Cephalometry in Orthodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Cephalometry in Orthodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.