Biological Mechanisms of Tooth Movement
Здесь есть возможность читать онлайн «Biological Mechanisms of Tooth Movement» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Biological Mechanisms of Tooth Movement
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Biological Mechanisms of Tooth Movement: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Biological Mechanisms of Tooth Movement»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
delivers a comprehensive reference for orthodontic trainees and specialists.
It is fully updated to include new chapters on personalized orthodontics as well as the inflammatory process occurring in the dental and paradental tissues. It is heavily illustrated throughout, making it easier for readers to understand and retain the information discussed within. The topics covered range from bone biology, the effects of mechanical loading on tissues and cells, genetics, tissue remodeling, and the effects of diet, drugs, and systemic diseases.
The Third Edition of
features seven sections that cover subjects such as:
The development of biological concepts in orthodontics, including the cellular and molecular biology behind orthodontic tooth movement Mechanics meets biology, including the effects of mechanical loading on hard and soft tissues and cells, and biological reactions to temporary anchorage devices Inflammation and orthodontics, including markers for tissue remodeling in the gingival crevicular fluid and saliva Personalized diagnosis and treatment based on genomic criteria, including the genetic influences on orthodontic tooth movement Rapid orthodontics, including methods to accelerate or decelerate orthodontic tooth movement Perfect for residents and PhD students of orthodontic and periodontal programs,
is also useful to academics, clinicians, bone biologists, and researchers with an interest in the mechanics and biology of tooth movement.
Biological Mechanisms of Tooth Movement — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Biological Mechanisms of Tooth Movement», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
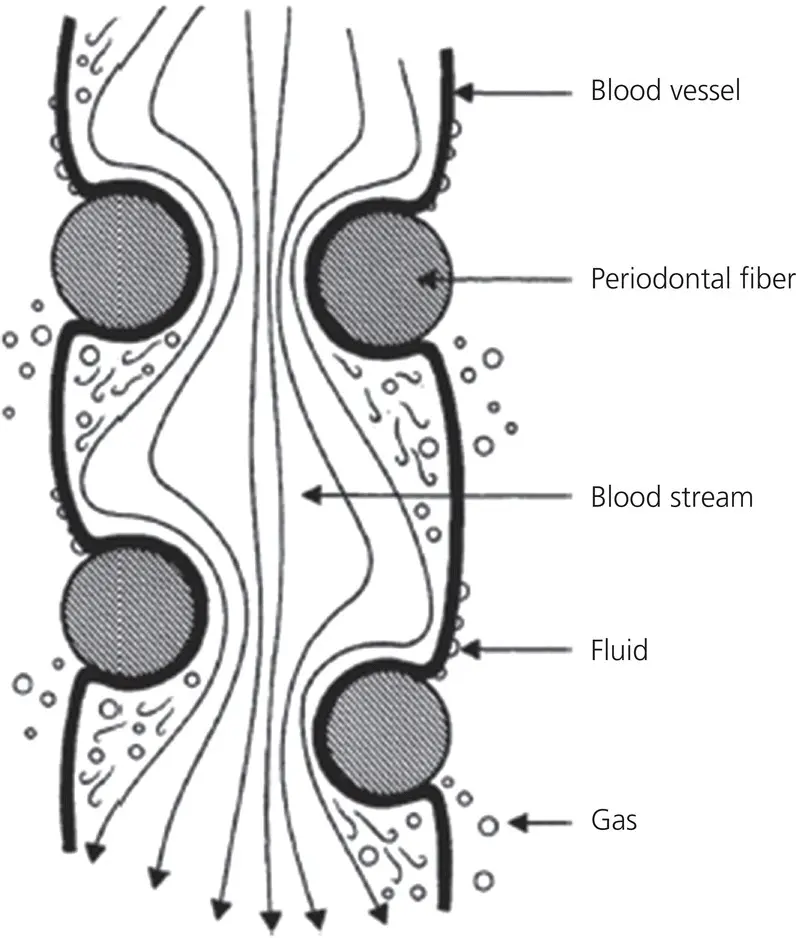
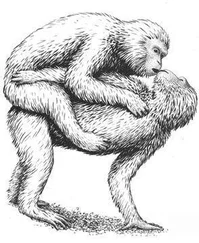
Figure 2.17 The constriction of a blood vessel by the periodontal fibers. The flow of blood in the vessels is occluded by the entwining periodontal fibers. Below the stenosis, the pressure drop gives rise to the formation of minute gas bubbles, which can diffuse through the vessel walls. Above the stenosis, fluid diffuses through the walls of the cirsoid aneurysms formed by the build‐up of pressure.
(Source: Bien, 1966. Reproduced with permission of SAGE Publications.)
With application of high sustained forces, as was the practice in the early era of orthodontics, capillary pressure will not be sufficient enough to counteract the effect and thus to replenish the fluid back to equilibrium. In this stage, the randomly running PDL fibers, which crisscross the blood vessels, tighten‐up, leading to compression, constriction of blood vessels, and leading to stenosis. This constriction point creates ballooning of the vessel wall above it, creating hydrodynamic pressure heads. Drawing support from Bernoulli’s principle, Bien explained the creation of a pressure drop in areas of stenosed blood vessels, leading to gas formation and sub‐atmospheric pressure. The gas bubbles formed might escape out of the capillaries and become lodged between bone spicules to create a favorable area for bone resorption. Bien attributed the large vacuoles seen in histologic sections of bone to be the escaped gas bubbles lodged there ( Figure 2.18). Furthermore, he associated the lack of cementum resorption with its smooth nature, containing fewer small radii of curvature, producing unfavorable areas for gas lodgment.
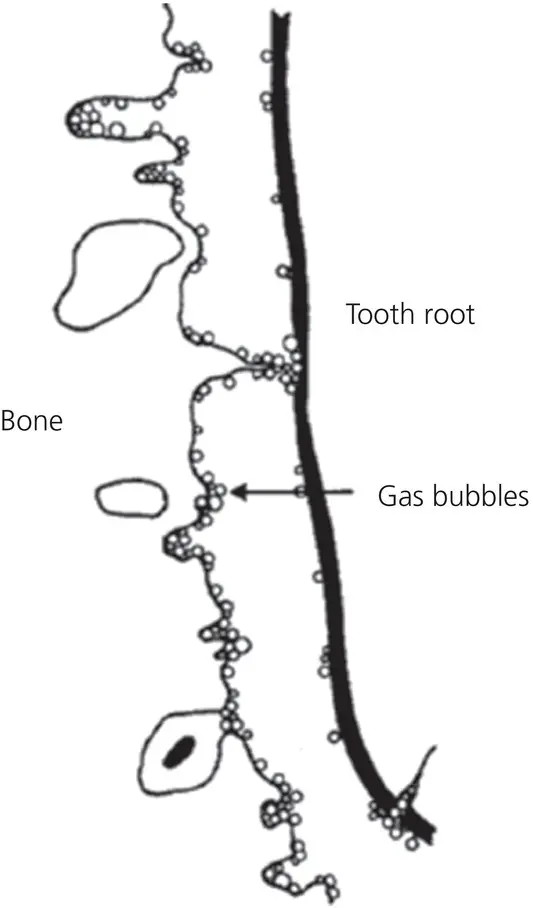
Figure 2.18 The lodgment of minute gas bubbles at small radii of curvature. The minute bubbles of gas, which diffuse through the blood vessel walls below the stenosis, lodge against the solid boundaries of tooth root and bone. Since there are many more areas of small radii of curvature in the bone, a greater number of gas bubbles may accumulate on the bone surface rather than on the root surface.
(Source: Bien, 1966. Reproduced with permission of SAGE Publications.)
The bone‐bending hypothesis
Baumrind (1969) explored the assumption that orthodontic forces bend the alveolar bone. He measured changes in PDL cell dimensions, metabolic activity, and fiber synthesis with the help of radioisotopes (tritiated thymine, uridine, and proline). While discussing the findings of his research, he highlighted a conceptual flaw in Schwarz’s pressure–tension hypothesis. He described the PDL as a continuous hydrostatic system, which, in accordance with Pascal’s law, dictates that force applied to this system is distributed equally to all regions of the PDL. He emphasized that the presence of fibers in the PDL does not modify the operation of this law, because of the concomitant existence of a continuous body of liquefied ground substance. He recognized that only part of the PDL, where differential pressures exist, as mentioned in the pressure–tension hypothesis, can be developed, is actually solid, i.e., bone, tooth, and discrete solid fractures of the PDL.
Kingsley (1881) and Farrar (1888) were the first to be credited for proposing the concept of bone bending as being an integral part of OTM. Farrar wrote in favor of this hypothesis: “Teeth move by one of two kinds of tissue changes in the alveolus … by the reduction of the alveolus through what is called absorption on one side of the tooth, followed by the growth of new supporting tissue on the other and by bending of the alveolar bone.” Kingsley and Farrar increased the force levels to such an extent that visible bending of alveolar bone could be observed, but several authors who followed this approach complained that their patients had experienced alveolar fractures. Because of this problem, and the influence of Oppenheim and his lectures in the Angle School, the pressure–tension hypothesis was uplifted, while the bone‐bending hypothesis was abandoned. Baumrind criticized the application of excessive forces for bone bending by describing them as “practical excesses of Kingsley and Farrar rather than theoretical misconceptions they had.” He revived the legacy of bone bending by basing it on Hook’s law (any solid body subjected to a load within its elastic limit will, if maintained in a static position, deform to a degree proportional to the magnitude of the applied force), the physical law of elasticity, which is fundamental to solid‐state mechanics, and stated that “alveolar bone does indeed deflect under mechanical loading and these can be produced by forces lower than those required to produce consequential changes in the PDL width.”
Proposing the bone‐bending hypothesis, Baumrind (1969) stated that “when orthodontic appliances are placed, forces delivered to the tooth are transmitted to all the tissues in the region of force application. In accordance with universally operating physical laws, each of the three types of structure in the area (tooth, PDL, and bone) is deformed. The amount of deformation produced in each material by a given force is a function of the elastic properties of that material. The elastic properties of the tooth itself have not been studied. Of the other two materials, I contend that the bone deforms far more readily than PDL.” When bone is held under mechanical forces, the remodeling and reorganization process is accelerated not only in the lamina dura, but also on the surface of every trabeculum within the corpus of the bone. The force/stress directed to the teeth will be dissipated by the development of stress lines in the deflected bone and becomes a major stimulus for altered biological activity, which in turn brings about adaptive changes. Baumrind claimed that his proposed hypothesis was complying with the basic rules of Wolff ’s law, as outlined by D’Arcy Thompson (1917), that strains are induced in bone by deflective forces within the elastic limit, and the tissue turnover and renewal are active so that bone can reorganize to accommodate the applied stress. In accordance with this theory, he could explain the phenomena behind
Relative slowness of en‐mass movements, and relative rapidity in the alignment of crowded anterior teeth.
The rapidity in which teeth can be moved into an extraction site.
The appearance of an axis of rotation beyond the apex of the incisors. The logic of the pressure–tension hypothesis makes it mandatory to have the axis between the apex and the alveolar crest.
The relative rapidity of tooth movement in children.
Baumrind also challenged the existence of the fluid dynamic hypothesis of Bien by stating that “there is simply no objective evidence for theories which postulate ‘squeezing out’ of tissue fluids from the PDL on the ‘pressure’ side. In any event, the PDL is a continuous system, so that if fluid were to be ‘squeezed out’ in one region it would have to be ‘squeezed out’ in all regions.”
The apposition and resorption of bone in response to its bending by orthodontic forces is evidently an attractive hypothesis, but it seems to contradict the current orthopedic dogma (Melsen, 1999), which states that “any mechanical compression stimulates bone formation and tension stimulates resorption.” Epker and Frost (1965) described the change in shape of the alveolar bone circumference resulting from stretching of the PDL fibers. This fiber stretching decreases the radius of the alveolar wall, i.e., bending of bone in the tension zone, where apposition of bone takes place. They attributed this response to a regional acceleratory phenomenon (RAP). Frost (1983) demonstrated that regional noxious stimuli of sufficient magnitude result in markedly accelerated reorganizing activity of osseous and soft tissues. It is a burst of localized remodeling process, which speeds up the healing potential, especially following the surgical wounding of cortical bone. Accordingly, any regional noxious stimulus of sufficient magnitude can evoke RAP. The extent of the affected region and intensity of the response vary directly with the magnitude and nature of the stimulus.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Biological Mechanisms of Tooth Movement»
Представляем Вашему вниманию похожие книги на «Biological Mechanisms of Tooth Movement» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Biological Mechanisms of Tooth Movement» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.