Biological Mechanisms of Tooth Movement
Здесь есть возможность читать онлайн «Biological Mechanisms of Tooth Movement» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Biological Mechanisms of Tooth Movement
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Biological Mechanisms of Tooth Movement: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Biological Mechanisms of Tooth Movement»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
delivers a comprehensive reference for orthodontic trainees and specialists.
It is fully updated to include new chapters on personalized orthodontics as well as the inflammatory process occurring in the dental and paradental tissues. It is heavily illustrated throughout, making it easier for readers to understand and retain the information discussed within. The topics covered range from bone biology, the effects of mechanical loading on tissues and cells, genetics, tissue remodeling, and the effects of diet, drugs, and systemic diseases.
The Third Edition of
features seven sections that cover subjects such as:
The development of biological concepts in orthodontics, including the cellular and molecular biology behind orthodontic tooth movement Mechanics meets biology, including the effects of mechanical loading on hard and soft tissues and cells, and biological reactions to temporary anchorage devices Inflammation and orthodontics, including markers for tissue remodeling in the gingival crevicular fluid and saliva Personalized diagnosis and treatment based on genomic criteria, including the genetic influences on orthodontic tooth movement Rapid orthodontics, including methods to accelerate or decelerate orthodontic tooth movement Perfect for residents and PhD students of orthodontic and periodontal programs,
is also useful to academics, clinicians, bone biologists, and researchers with an interest in the mechanics and biology of tooth movement.
Biological Mechanisms of Tooth Movement — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Biological Mechanisms of Tooth Movement», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
(Source: Sandstedt, 1904, 1905.).
(b) (Sandstedt’s Figure 10) A section through the middle third of the same tooth (in dogs, the pulp canal expands towards the middle third of the root before narrowing towards the apex). General remodeling activity at the bone–PDL interface is seen but evidence of the accelerated bone formation and resorption is absent. This area corresponds to the center of rotation of the tooth.
(Source: Sandstedt, 1904, 1905.)
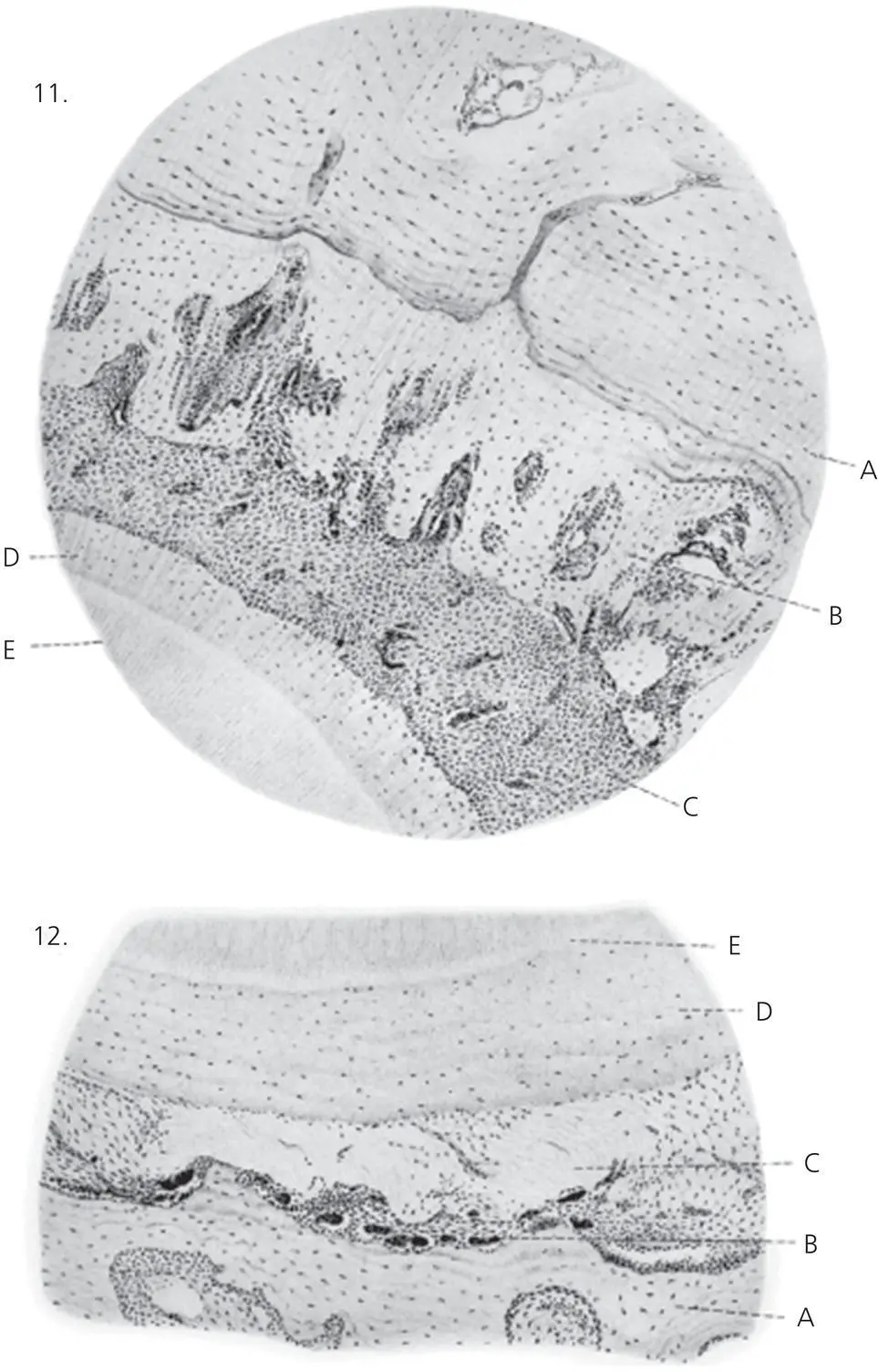
Figure 2.4 Plate IV A from Sandstedt’s original article. These sections show at a higher power the cellular and tissue changes in the PDL and alveolar bone at sites of presumptive tension and compression. Sandstedt’s Figure 11: tension in the PDL. A. Bone of the original alveolar wall. B. Newly laid‐down woven bone with vascular spaces clearly demarcated from the older lamellar bone. C. Highly vascular PDL. D. Cementum. E. Dentine. Sandstedt’s Figure 12: compression in the PDL. A. Bone of the original alveolar wall. B. Numerous dark‐staining osteoclasts lining the bone surface. C. The PDL in which the fibrillar structure has been lost and replaced by a glassy homogeneous or hyalinized tissue. D. Cementum. E. Dentine.
(Source: Sandstedt, 1904, 1905.)
Edward H. Angle, the father of modern orthodontics and follower of Wolff ’s law of bone adaptation to mechanical stress, was a proponent of the bone‐bending concept. He stated that the degree of bending of the alveolar bone is determined by the magnitude of the applied force, the age of the patient, and the direction of force application (Angle, 1907; Oppenheim, 1911). He advocated the bone remodeling hypothesis and suggested that resorption is seen in areas of pressure and traction, while deposition/apposition is for filling up of hollow areas created with this act. His writings were also in favor of the pressure hypothesis.
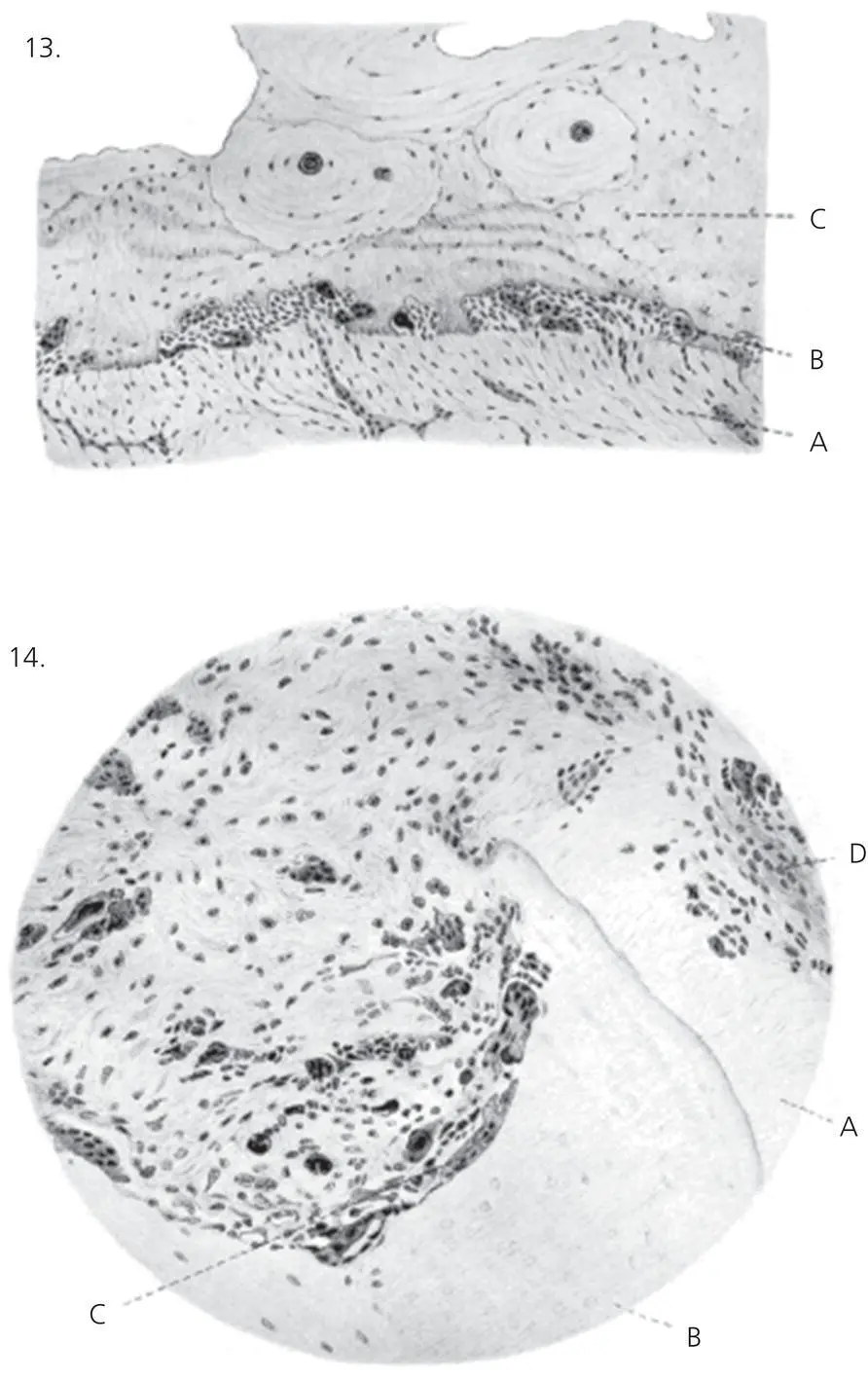
Figure 2.5 Plate IV B from Sandstedt’s original article. Sandstedt’s Figure 13: direct resorption. A. PDL at a compression site showing its normal fibrillar appearance. B. Numerous multinucleate osteoclasts in Howship’s lacunae are resorbing the surface of the bone. C. Cortical bone of the alveolus; two Haversian systems or secondary osteones are clearly visible. Sandstedt’s Figure 14. A. Hyalinized PDL. B. Although one cannot be absolutely sure, this section was likely to have been included to represent resorption of the root cementum at C by multinucleate giant cells. D. Unaffected periodontal ligament cells.
(Source: Sandstedt, 1904, 1905.)
Oppenheim’s transformation hypothesis
Oppenheim (1911) conducted OTM on a juvenile baboon, wherein he performed all sorts of tooth movements (labial, lingual, intrusion, extrusion, and rotation), with a split mouth design (where one side of the dental arch is operated upon, while the other side serves as control). He processed the jaw tissues histologically, and concluded that
The bony tissue, be it compact or cancelleous, reacts to pressure by a transformation of its entire architecture; this takes place by resorption of the bone present and deposition of new bony tissue; both processes occur simultaneously. Deposition finally preponderates over resorption. The newly formed bony spicules are arranged in the direction of the pressure [ Figure 2.6]. Increased pull has similarly resulted in addition of new bony tissue as a result, and simultaneous orientation of the spicules thereof in the direction of the pull [ Figure 2.7]. The entire transformation of the architecture and the orientation of the newly formed spongy bone spicules always occur so characteristically and lawfully, that we can say by the histological preparations in what manner the movements were accomplished. This characteristic transformation results only upon the application of very slight, physiological‐like influences. Should the force be too strong, the result will be such serious injuries to the periosteum, due to the disturbances in circulation, that there will be no typical reaction of the bony cells.
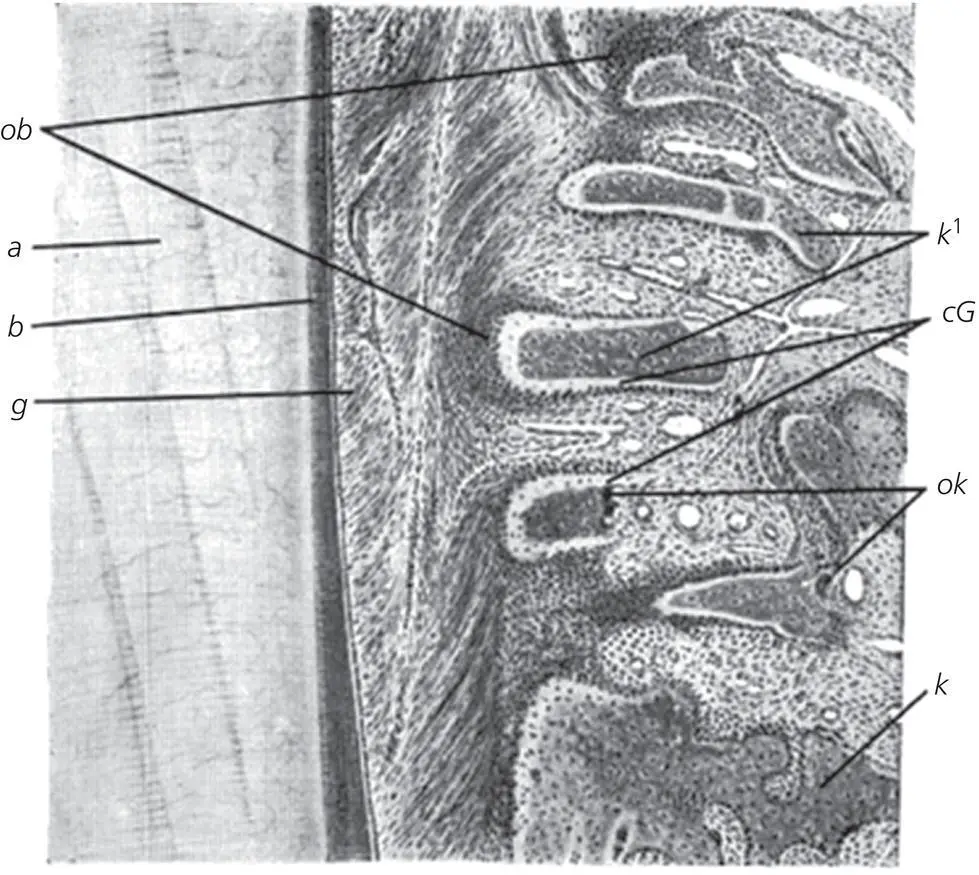
Figure 2.6 Histologic section from the original article by Oppenheim (1911). Lingual movement; lingual side of the PDL, where it forms compression. The individual newly formed bone spicules ( k 1) have arranged themselves in the direction of the force, perpendicular to the long axis of the tooth. The ends of the spicules directed toward the tooth: the ends subjected directly to the pressure show broad, uncalcified zones (cG), which are surrounded by densely arranged rows of osteoblasts ( ob ). At the ends of the spicules directed from the tooth, occasionally numerous osteoclasts are seen. a , dentine; b , cementum; g , PDL; ok , osteoclasts; nearer to the apex of the root old unchanged bone ( k ).
(Source: Oppenheim, 1911. Reproduced with permission of Oxford University Press.)
Oppenheim substantiated his findings by drawing support from Wolff ’s law, and his investigations could not find any injury in the PDL. He concluded that, in OTM, all mechanical forces applied to a tooth are absorbed by the PDL, and at times he could observe a hypertrophy to withstand the increased demand placed upon it. Unlike Sandstedt, Oppenheim reported on seeing no hyalinization or undermining resorption in his experimental material. He further wrote that “The vitality of the periosteum suffers no injury during the application of “physiological forces,” even on compression of the PDL to a third of its original thickness. It may be exposed to slight hemorrhages, to occasional constriction in the lumen, or disappearance of the vessels, but the staining ability of the cell nuclei is retained, and no disintegration can be demonstrated by any photographs.
The pressure–tension hypothesis
Schwarz (1932), working along the same lines as both Sandstedt and Oppenheim, formulated the “pressure–tension hypothesis” of OTM. It is postulated that in sites of compression in the PDL, it displays disorganization and diminution of fiber production. Here, cell replication decreases, seemingly as a result of vascular constriction. In contrast, in PDL tension sites, stimulation produced by stretching of fiber bundles results in an increase in cell replication. Schwarz detailed the concept further by correlating the tissue response to the magnitude of the applied force with the capillary blood pressure and categorized it as four degrees of biologic effect:
First degree of biologic effect. The force is of such a short duration or so slight that no reaction whatsoever is caused in the periodontium.
Second degree of biologic effect ( Figure 2.8). The force is gentle, speaking biologically; it remains below the pressure in the blood capillaries, i.e., less than 20–26 g for 1 cm2 of root surface, but it is nevertheless sufficient to cause resorption in the alveolar bone at the regions of pressure in the PDL. After the force ceases there will be anatomic and functional resolution of integrity of the PDL and alveolar bone without resorption of dental roots. Figure 2.7 Elongation from the original article by Oppenheim (2011). Apex of the root (a). The spongy bone spicules at the root apex appear as long, thin, buttresses, stretching from the depth toward the root apex (k1), their tops and sides being enclosed by narrow uncalcified zones and strong layers of osteoblasts (ob). ok, osteoclasts.(Source: Oppenheim, 1911. Reproduced with permission of Oxford University Press.)
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Biological Mechanisms of Tooth Movement»
Представляем Вашему вниманию похожие книги на «Biological Mechanisms of Tooth Movement» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Biological Mechanisms of Tooth Movement» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.