Biological Mechanisms of Tooth Movement
Здесь есть возможность читать онлайн «Biological Mechanisms of Tooth Movement» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Biological Mechanisms of Tooth Movement
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Biological Mechanisms of Tooth Movement: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Biological Mechanisms of Tooth Movement»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
delivers a comprehensive reference for orthodontic trainees and specialists.
It is fully updated to include new chapters on personalized orthodontics as well as the inflammatory process occurring in the dental and paradental tissues. It is heavily illustrated throughout, making it easier for readers to understand and retain the information discussed within. The topics covered range from bone biology, the effects of mechanical loading on tissues and cells, genetics, tissue remodeling, and the effects of diet, drugs, and systemic diseases.
The Third Edition of
features seven sections that cover subjects such as:
The development of biological concepts in orthodontics, including the cellular and molecular biology behind orthodontic tooth movement Mechanics meets biology, including the effects of mechanical loading on hard and soft tissues and cells, and biological reactions to temporary anchorage devices Inflammation and orthodontics, including markers for tissue remodeling in the gingival crevicular fluid and saliva Personalized diagnosis and treatment based on genomic criteria, including the genetic influences on orthodontic tooth movement Rapid orthodontics, including methods to accelerate or decelerate orthodontic tooth movement Perfect for residents and PhD students of orthodontic and periodontal programs,
is also useful to academics, clinicians, bone biologists, and researchers with an interest in the mechanics and biology of tooth movement.
Biological Mechanisms of Tooth Movement — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Biological Mechanisms of Tooth Movement», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
During OTM, cellular activities in sites of PDL tension are meant to narrow the widened space created by the movement of the dental root away from the alveolar bone. This stretching of the PDL affects both the cells and their extracellular matrix (ECM). The stretched cells detach themselves from their surrounding ECM, then reattach, and engage in a variety of functions commensurate with returning the width of the PDL to its original dimensions. These functions include proliferation, differentiation, synthesis and secretion of autocrine and paracrine molecules, and new ECM components. Some of these components are mineralizable and will eventually become the new layer of bone that covers the alveolar surface that faces the stretched PDL. The new bone first appears as fingerlike projections, which grow along the stretched PDL fibers, perpendicular to the surface of the old alveolar bone. The force‐induced strains alter the PDL’s nervous network, vascularity, and blood flow, resulting in local synthesis and/or release of various key molecules, such as vasoactive neurotransmitters, cytokines, growth factors, colony‐stimulating factors, and arachidonic acid metabolites. These molecules evoke a plethora of cellular responses by many cell types in and around teeth, providing a favorable microenvironment for tissue deposition or resorption (Davidovitch, 1991; Krishnan and Davidovitch, 2006).
The studies performed in the early years of the twentieth century were mainly directed towards analyzing the histological changes in paradental tissues following short‐term and long‐term OTM. Those studies revealed extensive cellular activities in the mechanically stressed PDL, involving neurons, immune cells, fibroblasts, endothelial cells, osteoblasts, osteoclasts, osteocytes, and endosteal cells. Moreover, mechanical stresses were found to alter the structural properties of tissues at the cellular, molecular, and genetic levels. The rapid reactions occurring at the initial stage of mechanotherapy, and slower adaptive changes at the later stages of treatment, have attracted increasing attention. This chapter addresses the evolutionary traits of the development of concepts pertaining to the biology of OTM.
Hypotheses about the biological nature of OTM: The conceptual evolution
OTM is the result of a biological response to interference in the physiological equilibrium of the dentofacial complex by an externally applied force (Proffit, 2013). The biological foundation of force‐induced tooth movement, along with some concepts related to it, has been extensively investigated since the onset of the twentieth century. From the classic reports by Sandstedt in 1904 ( Figure 2.1), the race was set for exploring the biological foundations of OTM, using histology, radiology, and clinical observations as the main investigative tools. A list of the then prevailing hypotheses aimed at explaining the biological reasons for OTM is presented below:
The old pressure hypothesis of Schwalbe–Flourens, which postulated that pressure moves teeth, preceded the concept that alveolar bone resorption takes place on one side of the dental root, while deposition occurs on the opposite side, until the pressure is eliminated. Hecht (1900), Sandstedt (1904), Pfaff (1906), and Angle (1907) supported this hypothesis (Oppenheim, 1911).
Based on his vast clinical experience, Kingsley (1881) stated that slow OTM is associated with favorable tissue‐remodeling changes (resorption and deposition of alveolar bone), while quick movements displace the entire bony lamellae along with the teeth, while retaining their functional and structural integrity. He attributed these features to the elasticity, compressibility, and flexibility of bone tissue. This report is one of the first written explanations for the biological basis of OTM, although it is not frequently cited (Oppenheim, 1911).
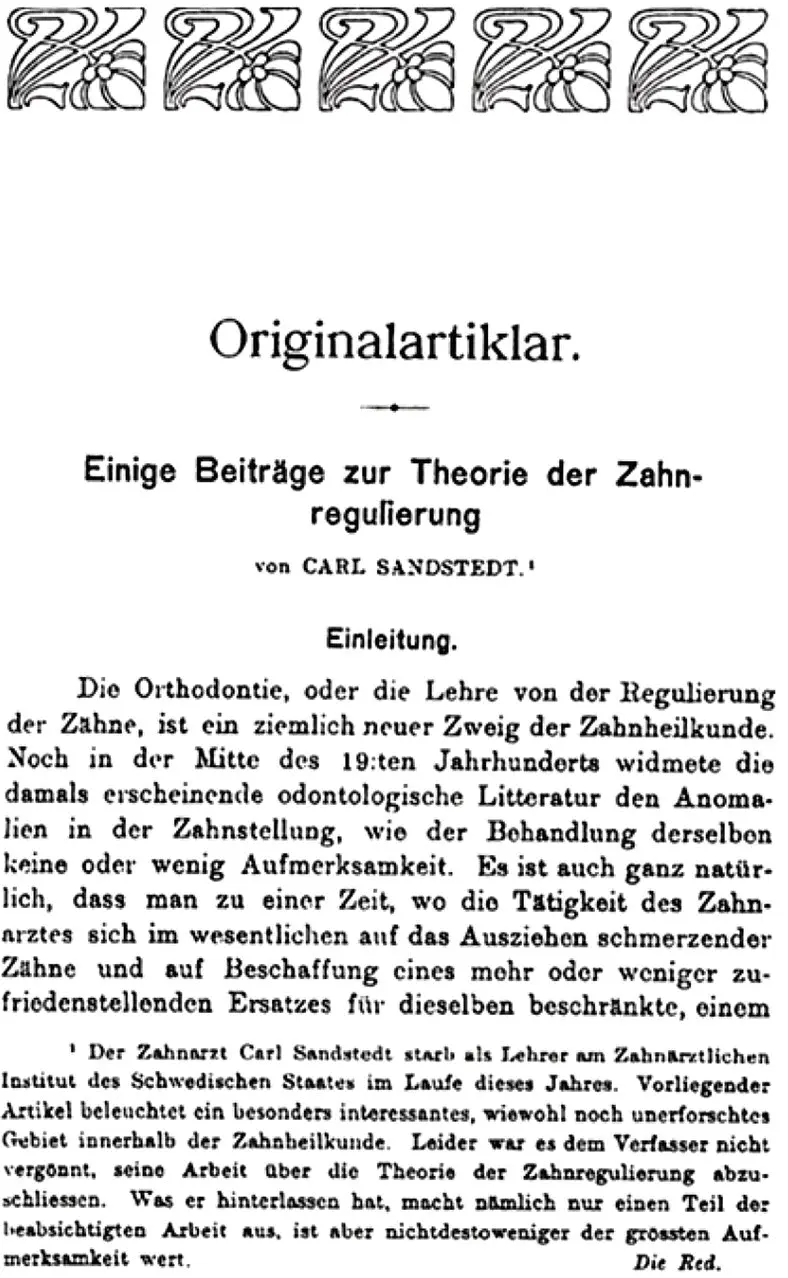
Figure 2.1 Page 1 from Sandstedt’s original article on histological studies of tooth movement published in 1904.
(Source: Sandstedt, 1904, 1905.)
Walkhoff’s hypothesis on the biology of OTM
Soon after Kingsley’s contribution, Walkhoff (1890) stated that “movement of a tooth consists in the creation of different tensions in the bony tissue, its consolidation in the compensation of these tensions.” Walkhoff’s hypothesis was largely based on the elasticity, flexibility, and compressibility of bone, and the transposition of the histological elements (such as the PDL). He also stated that alveolar bone, after all the remodeling changes, maintains its thickness, due to transformation or apposition of bone during the consolidating (retentive) period (Walkhoff, 1891). He emphasized the importance of retention, stating that “osteoid tissue has nothing to do with tooth movement. If we were to remove the retaining devices already after a few weeks from corrected protruding front teeth like from a fractured bone after the formation of a callus, we had only to deal with failures.” The propositions by Walkhoff were based solely on his clinical observations and practical knowledge but lacked the backing of histological evidence.
In 1900, Hecht described a cartilaginous transformation of the bone and rupture of bony spicules surrounding teeth during OTM. He interpreted this situation as an indication of severe changes and leaned upon Schwalbe–Flourens’ pressure hypothesis (Oppenheim, 1911) to substantiate his interpretation. However, Oppenheim argued against this viewpoint, stating that the severe changes, which Hecht had observed, might have been the result of the application of excessive force (Oppenheim, 1911). In any case, Hecht did not support his assumptions with any histological evidence.
Histological examination of paradental tissues during OTM was reported for the first time by Sandstedt (1904), who tipped teeth uncontrollably in dogs, and later studied their tissues by light microscopy (Figures ). In these sections he observed areas of pressure and tension in the PDL, and necrosis or hyalinization zones in the PDL at sites of great compression. Oppenheim (1911), while trying to duplicate those experiments, could not find any thrombosis in vessels or hyalinization in the PDL. He speculated that the lack of necrosis in his own experiment might have been due to the use of light force, in contrast to the heavy forces used by Sandstedt.
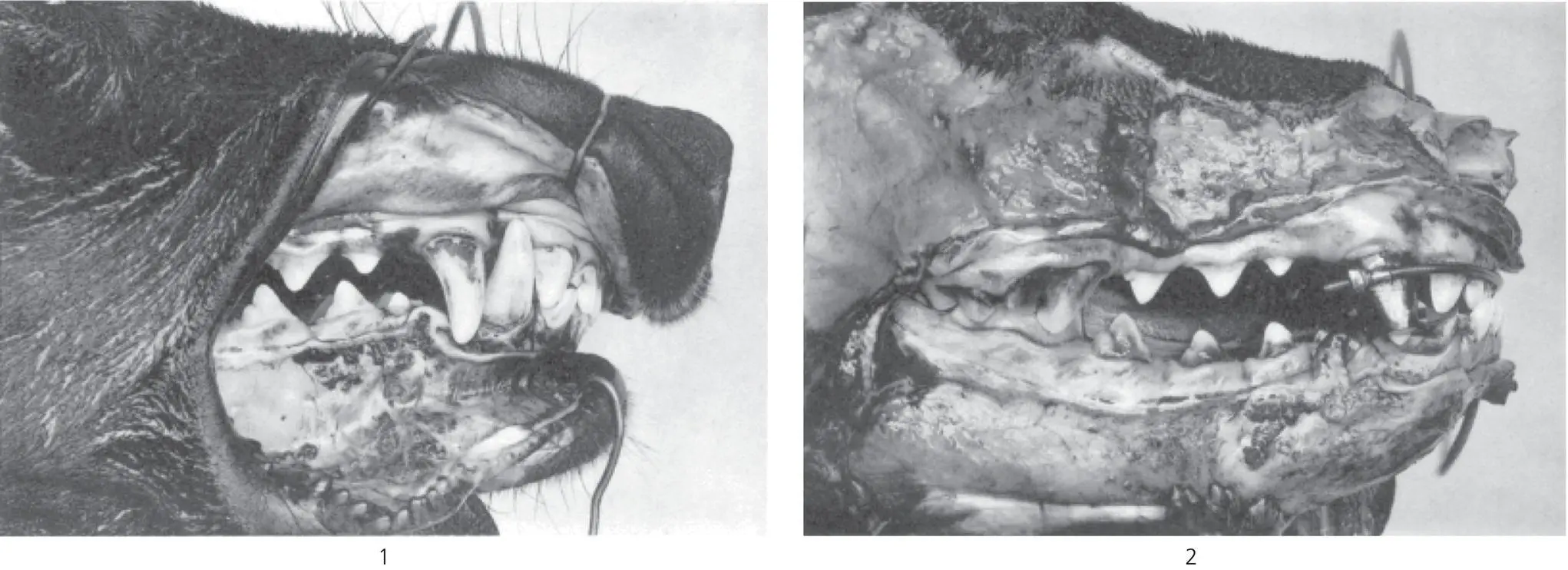
Figure 2.2 Plate I from Sandstedt’s original article showing photographs of the control (1) and experimental (2) dogs at sacrifice. The mandibular canines were removed to allow the movement of the maxillary teeth. The appliance consisted of an archwire inserted into tubes attached to bands on the upper canines; distal to the tubes was a screw mechanism, which, when tightened, moved the incisors lingually and the canines mesially.
(Source: Sandstedt, 1904, 1905).
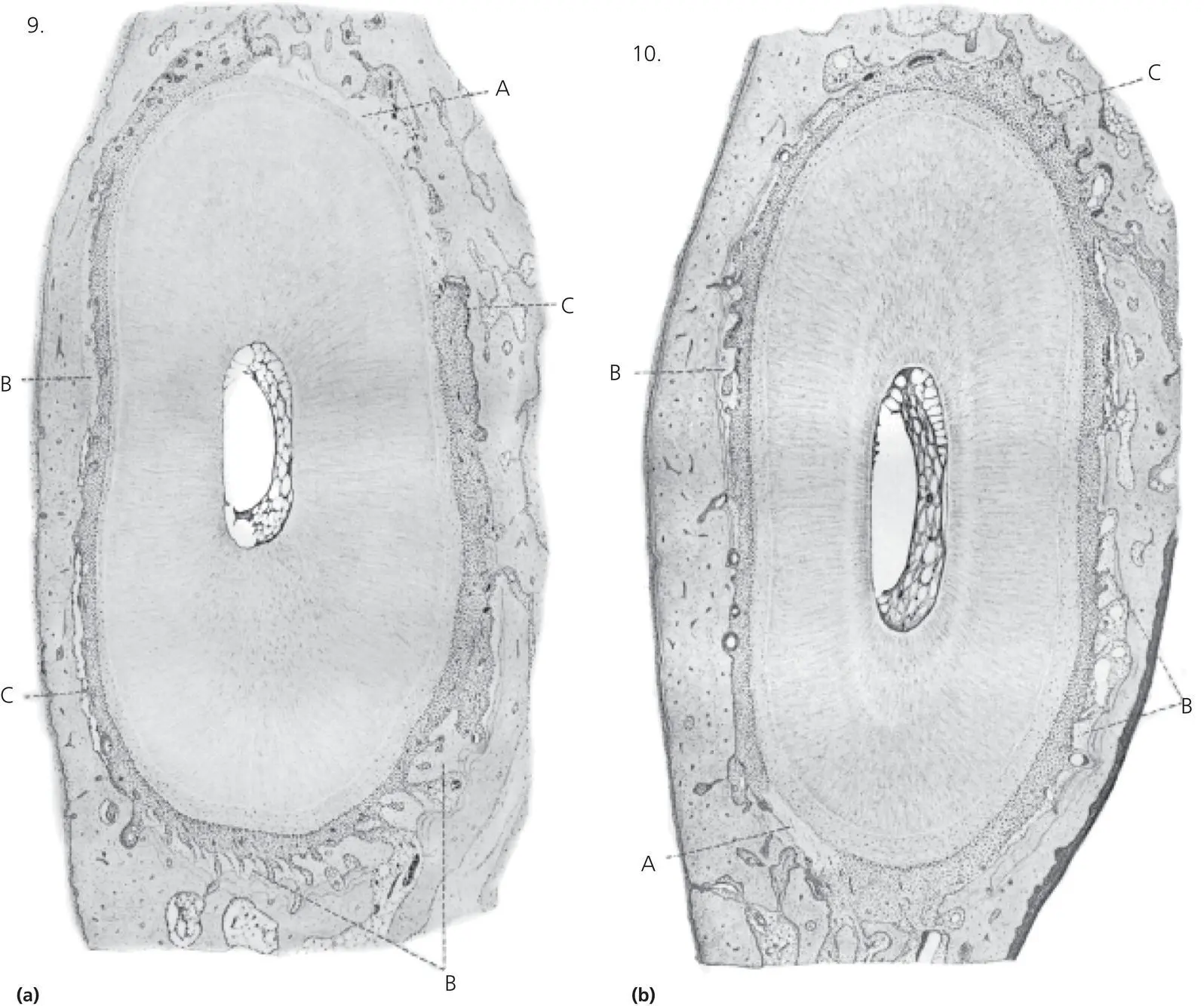
Figure 2.3 Plate III from Sandstedt’s original article showing horizontal sections through the right maxillary canine; the direction of movement is towards the top.
(Source: Sandstedt, 1904, 1905.).
(a) (Sandstedt’s Figure 9.) A section cut in close proximity to the alveolar rim. A. At the site of presumptive compression, the PDL shows the glassy appearance characteristic of hyalinization, with osteoclasts undermining the adjacent alveolar wall. B. On the buccal side of the root, a thin layer of lighter staining new bone is demarcated from the old bone by a von Ebner (reversal) line. At the bottom, new bone takes the form of lighter staining bony trabeculae of woven bone orientated in the direction of pull. C. On the right side, osteoclasts are resorbing the alveolar wall; on the left, the detachment of the PDL from the bone is the result of a tear during sectioning.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Biological Mechanisms of Tooth Movement»
Представляем Вашему вниманию похожие книги на «Biological Mechanisms of Tooth Movement» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Biological Mechanisms of Tooth Movement» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.