Salivary Gland Pathology
Здесь есть возможность читать онлайн «Salivary Gland Pathology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Salivary Gland Pathology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Salivary Gland Pathology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Salivary Gland Pathology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
now features case presentations to place the information in context, as well as additional treatment algorithms in each chapter to assist in clinical decision making. Written by highly respected clinicians, educators, and researchers with extensive expertise in oral and maxillofacial surgery, this authoritative resource:
Reviews the etiology, diagnosis, and treatment of all salivary gland pathologies, with detailed explanations and hundreds of full-color clinical images Incorporates new information on the taxonomy of salivary gland tumors, neoplastic and non-neoplastic entities, image guided biopsies of salivary gland lesions, and complications in traditional and non-traditional forms of salivary gland surgery Offers expanded coverage of histopathology, including classification, grading, and staging of salivary gland tumors Features up-to-date chapters on anatomy and physiology, imaging, cysts, systemic diseases, tumors, trauma, and innovative salivary gland surgical techniques Includes a discussion of meta-analyses and systematic reviews to support evidence-based practice remains the definitive resource for oral and maxillofacial surgeons, otolaryngologists, head and neck surgeons, and general surgeons as well as their residents providing care for patients with salivary gland pathology.
Salivary Gland Pathology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Salivary Gland Pathology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The shape of the parotid gland is variable. Often it is triangular with the apex directed inferiorly. However, on occasion, it is essentially of even width and occasionally it is triangular with the apex superiorly. On average, the gland is 6 cm in length with a maximum of 3.3 cm in width. In 20% of subjects, a smaller accessory lobe arises from the upper border of the parotid duct approximately 6 mm in front of the main gland. This accessory lobe overlies the zygomatic arch.
The gland is surrounded by a fibrous capsule previously thought to be formed from the investing layer of deep cervical fascia. This fascia passes up from the neck and was thought to split to enclose the gland. The deep layer is attached to the mandible and the temporal bone at the tympanic plate and styloid and mastoid processes (McMinn et al. 1984; Berkovitz and Moxham 1988; Williams 1995; Ellis 1997). Recent investigations suggest that the superficial layer of the parotid capsule is not formed in this way, but is part of the superficial musculo‐aponeurotic system (SMAS) (Mitz and Peyronie 1976; Jost and Levet 1983; Wassef 1987; Thaller et al. 1989; Zigiotti et al. 1991; Gosain et al. 1993; Flatau and Mills 1995). Anteriorly, the superficial layer of the parotid capsule is thick and fibrous but more posteriorly it becomes a thin translucent membrane. Within this fascia are scant muscle fibers running parallel with those of the platysma. This superficial layer of the parotid capsule appears to be continuous with the fascia overlying the platysma muscle. Anteriorly it forms a separate layer overlying the masseteric fascia which is itself an extension of the deep cervical fascia. The peripheral branches of the facial nerve and the parotid duct lie within a loose cellular layer between these two sheets of fascia. This observation is important in parotid surgery. When operating on the parotid gland, the skin flap can either be raised in the subcutaneous fat layer or deep to the SMAS layer. The SMAS layer itself can be mobilized as a separate flap and can be used to mask the cosmetic defect following parotidectomy by reattaching it firmly to the anterior border of the sternocleidomastoid muscle as an advancement flap (Meningaud et al. 2006).
The parotid capsule develops relatively late after the lymphoid tissue develops within the mesenchyme of the gland (Goldenberg et al. 2000). For this reason, the lymph nodes associated with the parotid gland are intraglandular as opposed to the extraglandular lymph nodes associated with the submandibular and sublingual salivary glands, in which the capsule forms earlier in their development.
Where the deep aspect of the superficial lobe overlies branches of the facial nerve, the capsule becomes very thin or even nonexistent, resulting in acinar tissue lying in direct contact with the nerve fibers.
The superior border of the parotid gland (usually the base of the triangle) is closely molded around the external acoustic meatus and the temporomandibular joint. An avascular plane exists between the gland capsule and the cartilaginous and bony acoustic meatus ( Figure 1.2). The inferior border (usually the apex) is at the angle of the mandible and often extends beyond this to overlap the digastric triangle where it may lie very close to the posterior pole of the submandibular salivary gland. The anterior border just overlaps the posterior border of the masseter muscle and the posterior border overlaps the anterior border of the sternocleidomastoid muscle.
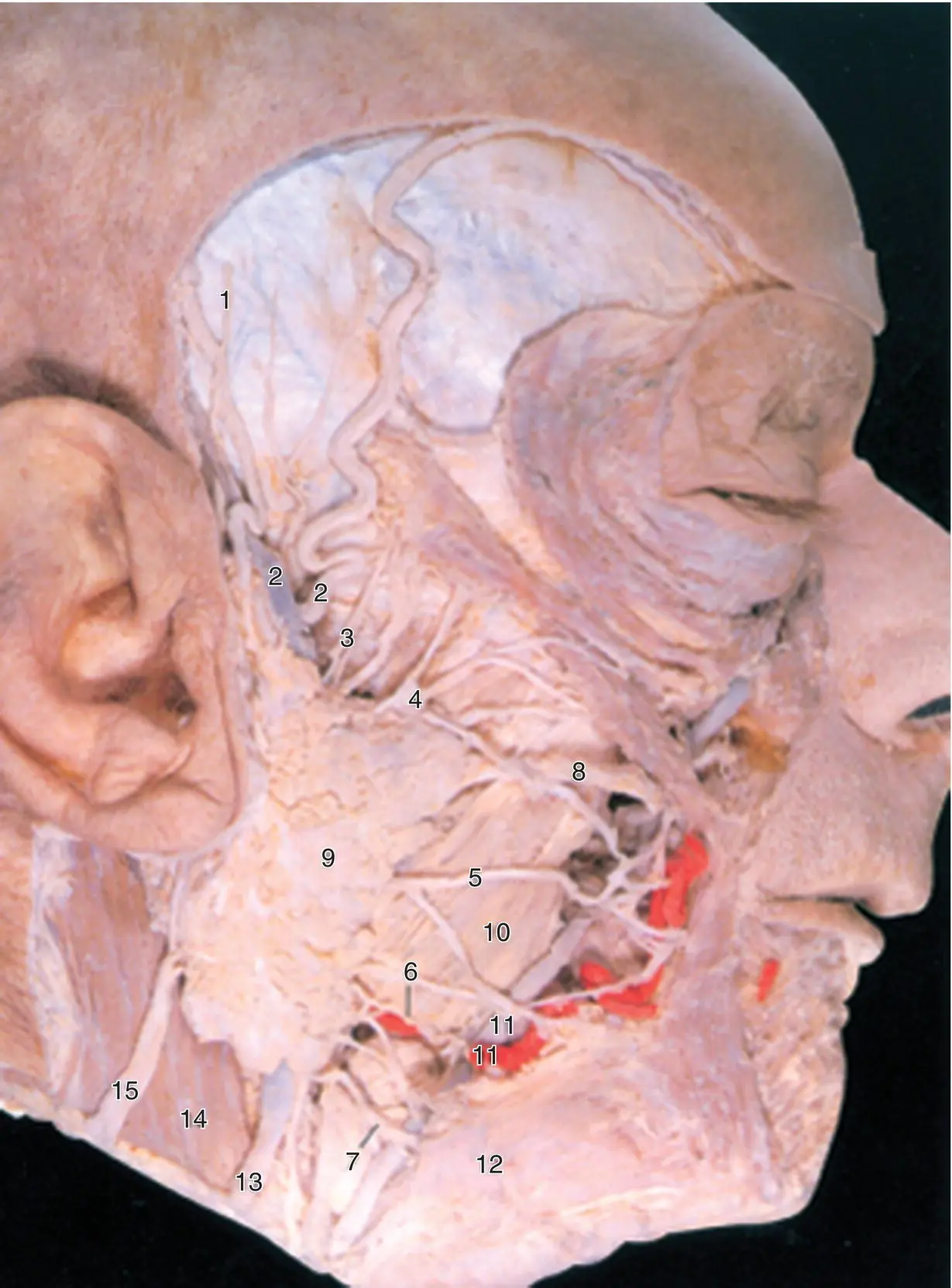
Figure 1.2. The parotid gland and associated structures.
Source: Published with permission, Martin Dunitz, London, Langdon JD, Berkowitz BKB, Moxham BJ, editors, Surgical Anatomy of the Infratemporal Fossa. DOI: 10.1002/9781118949139.ch1.
The superficial surface of the gland is covered by skin and platysma muscle. Some terminal branches of the great auricular nerve also lie superficial to the gland. At the superior border of the parotid, lie the superficial temporal vessels with the artery in front of the vein. The auriculotemporal branch of the mandibular nerve runs at a deeper level just behind the superficial temporal vessels.
The branches of the facial nerve emerge from the anterior border of the gland. The parotid duct also emerges to run horizontally across the masseter muscle before piercing the buccinator muscle anteriorly to end at the parotid papilla. The transverse facial artery (a branch of the superficial temporal artery) runs across the area parallel to and approximately 1 cm above the parotid duct. The anterior and posterior branches of the facial vein emerge from the inferior border.
The deep (medial) surface of the parotid gland lies on those structures forming the parotid bed. Anteriorly the gland lies over the masseter muscle and the posterior border of the mandibular ramus from the angle up to the condyle. As the gland wraps itself around the ramus, it is related to the medial pterygoid muscle at its insertion on to the deep aspect of the angle. More posteriorly, the parotid is molded around the styloid process and the styloglossus, stylohyoid, and stylopharyngeus muscles from below upwards. Behind this, the parotid lies on the posterior belly of the digastric muscle and the sternocleidomastoid muscle. The digastric and the styloid muscles separate the gland from the underlying internal jugular vein, the external and internal carotid arteries and the glossopharyngeal, vagus, accessory, and hypoglossal nerves and the sympathetic trunk.
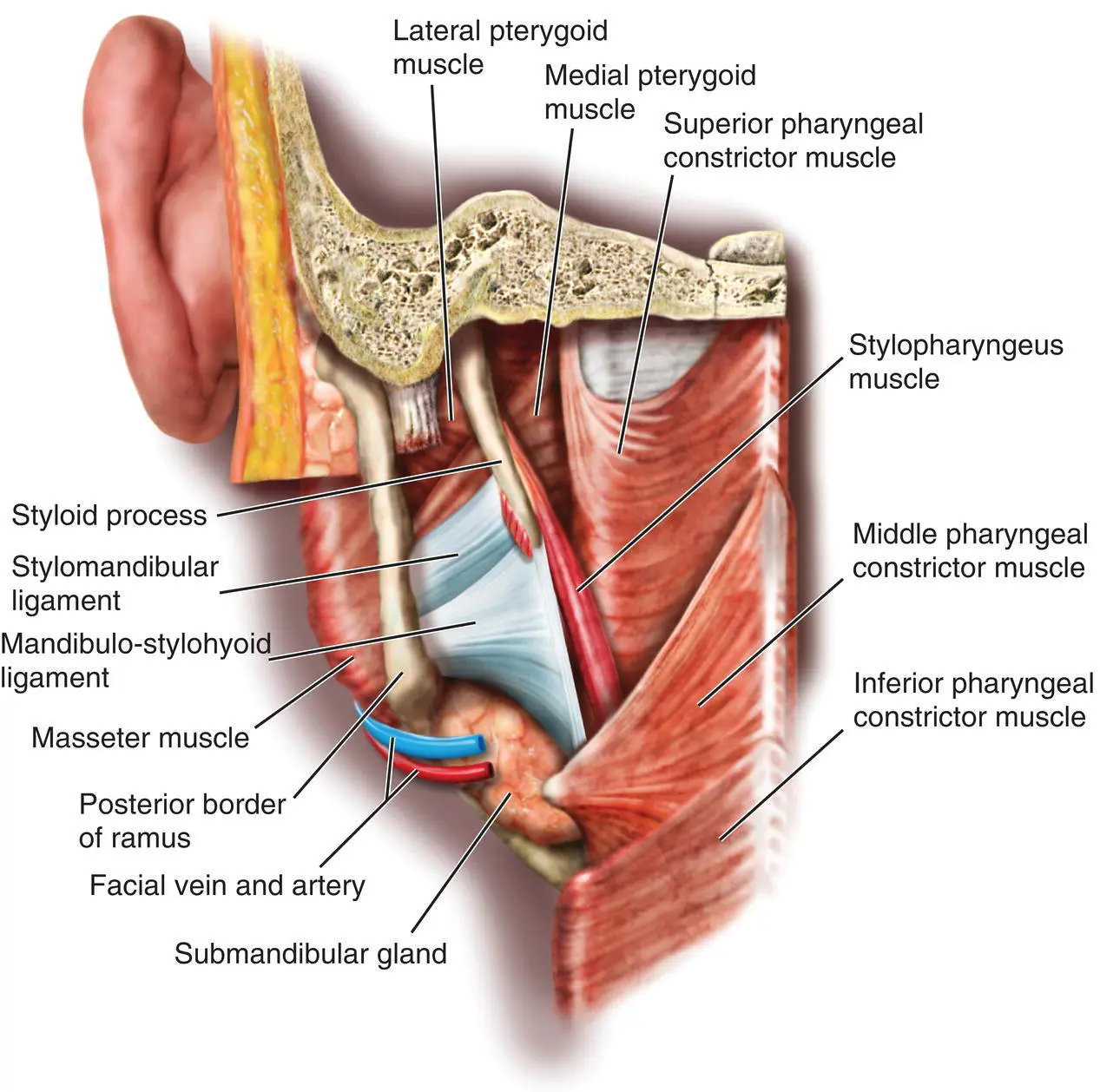
Figure 1.3. The mandibulo‐stylohyoid ligament.
The fascia that covers the muscles in the parotid bed thickens to form two named ligaments ( Figure 1.3). The stylomandibular ligament passes from the styloid process to the angle of the mandible. The mandibulo‐stylohyoid ligament (the angular tract) passes between the angle of the mandible and the stylohyoid ligament. Inferiorly, it usually extends down to the hyoid bone. These ligaments are all that separates the parotid gland anteriorly from the posterior pole of the superficial lobe of the submandibular gland.
CONTENTS OF THE PAROTID GLAND
Facial Nerve
From superficial to deep, the facial nerve, the auriculotemporal nerve, the retromandibular vein, and the external carotid artery pass through the substance of the parotid gland.
The facial nerve exits the skull base at the stylomastoid foramen. The surgical landmarks are important ( Figure 1.4). To expose the trunk of the facial nerve at the stylomastoid foramen, the dissection passes down the avascular plane between the parotid gland and the external acoustic canal until the junction of the cartilaginous and bony canals is palpated. A small triangular extension of the cartilage points toward the facial nerve as it exits the foramen (Langdon 1998b). This is the so‐called tragal pointer. The main trunk of the nerve lies approximately 13.6 mm from this landmark but there is considerable variation (Ji et al. 2018). The nerve lies about 9 mm from the posterior belly of the digastric muscle where the digastric passes deep to the sternocleidomastoid muscle, and 11 mm from the bony external meatus (Holt 1996). The facial nerve then passes downwards and forwards over the styloid process and associated muscles for about 1.3 cm before entering the substance of the parotid gland (Hawthorn and Flatau 1990). The first part of the facial nerve gives off the posterior auricular nerve supplying the auricular muscles and also branches to the posterior belly of the digastric and stylohyoid muscles.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Salivary Gland Pathology»
Представляем Вашему вниманию похожие книги на «Salivary Gland Pathology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Salivary Gland Pathology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.