Interpretation Basics of Cone Beam Computed Tomography
Здесь есть возможность читать онлайн «Interpretation Basics of Cone Beam Computed Tomography» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Interpretation Basics of Cone Beam Computed Tomography
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Interpretation Basics of Cone Beam Computed Tomography: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Interpretation Basics of Cone Beam Computed Tomography»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Enables rapid reference to common CBCT findings, with multiple images for each finding Features a streamlined framework that makes relevant information easier to find and apply in dental practice Offers hundreds of new images to aid in correctly identifying findings Contains new and updated content, including expanded coverage of CBCT and implants Provides sample reports and explains how they are used in day-to-day clinical practice
remains a must-have resource for all dental practitioner and specialists who use CBCT, dental students in radiology interpretation courses, and residents beginning to use CBCT in their specialty.
Interpretation Basics of Cone Beam Computed Tomography — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Interpretation Basics of Cone Beam Computed Tomography», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
2010 Position Paper
There were two main imaging goals from the 2010 paper – field of view (FOV) and resolution/voxel size. A small/limited FOV and a resolution/voxel size of 0.2 mm or smaller is recommended. This combination allows better visualization for small changes to the periodontal ligament space, bone, and teeth. When using CBCT, it should not be used for routine use and should be based on a patient’s history and clinical examination. Before capturing a CBCT scan, it is important to receive patient consent and explain the risks and benefits of the imaging modality. Last, the entire CBCT volume must be interpreted.
2015/2016 Update
The updated position paper gives 14 case examples and whether a limited FOV CBCT or intraoral 2D imaging is recommended. They are separated into different categories: diagnosis, initial treatment, nonsurgical treatment, surgical retreatment, special conditions, and outcome assessment.
Diagnosis
1 = Intraoral radiographs should be considered for the evaluation of endodontic patients.
2 = Limited FOV CBCT should be considered when there are nonspecific clinical signs or symptoms with an untreated or previously endodontically treated tooth.
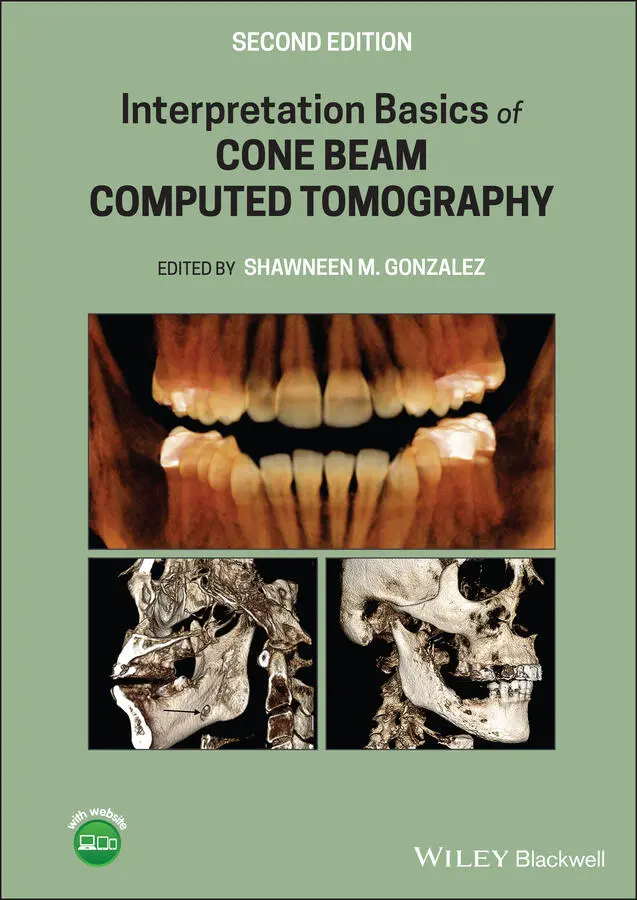
CBCT imaging has increased sensitivity in the detection of periapical pathosis ( Figure 2.1) compared to intraoral radiographs. In the presence of clinical signs with the absence of intraoral radiographic findings, a CBCT may be recommended to rule out or rule in possible periapical pathosis. It is important to thoroughly check all of the teeth on a scan because early periapical pathosis has been noted on CBCT prior to detection on intraoral radiographs. Sagittal and cross‐sectional views are the recommended views for detecting periapical pathosis.
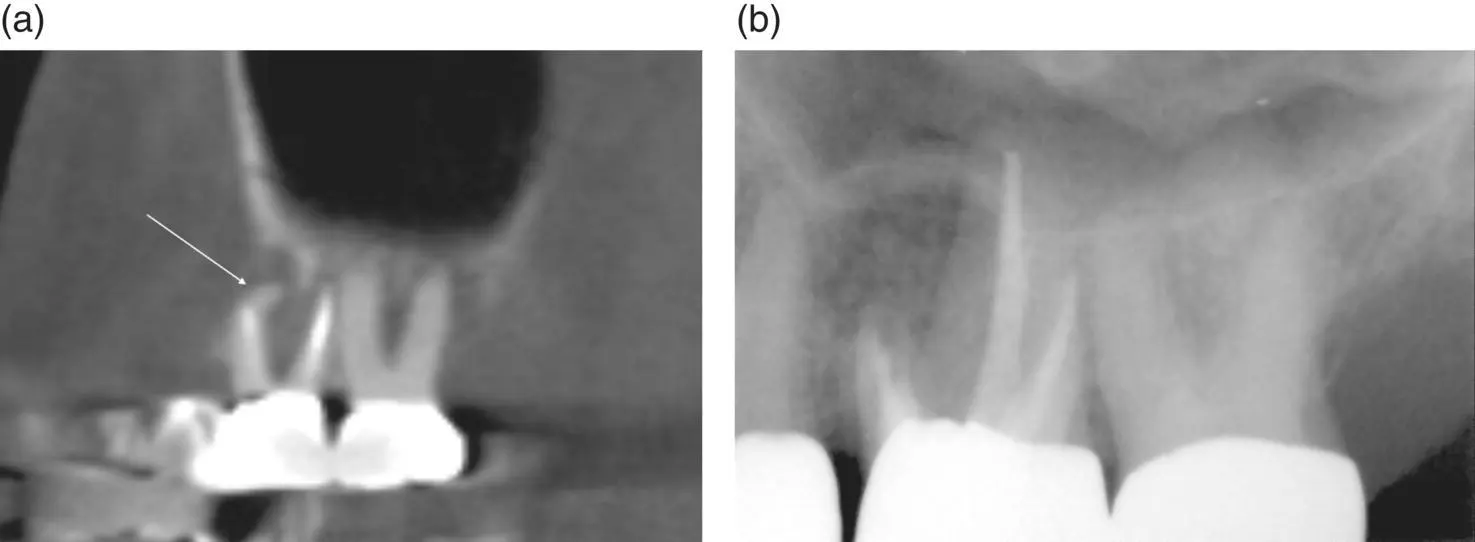
Figure 2.1. (a) Sagittal view showing a distal dilaceration of the mesio‐buccal root of the maxillary first molar with a short endodontic filling and rarefying osteitis (white arrow). (b) Periapical radiograph showing a resulting apicoectomy after the findings on the CBCT scan.
Initial Treatment
3 = Limited FOV CBCT should be considered when evaluating teeth with potential extra canals or complex morphology (excludes maxillary incisors) ( Figure 2.2).

Figure 2.2. Coronal view showing a maxillary premolar with an unfilled palatal root (white arrow) and apical rarefying osteitis.
4 = Limited FOV CBCT should be considered to identify and localize calcified canals.
5 = Intraoral radiographs should be considered for immediate postoperative evaluation.
Nonsurgical Treatment
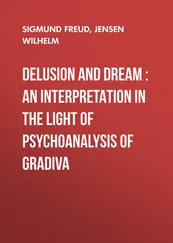
6 = Limited FOV CBCT should be considered if the clinical exam and intraoral radiographs are inconclusive for detecting a vertical root fracture.
Vertical root fractures are difficult to diagnose on intraoral radiographs with localized bone changes visualized first ( Figure 2.3). The bone changes typically present with J‐shaped bone loss around the root with the fracture. CBCT imaging has increased sensitivity in detecting vertical and horizontal root fractures ( Figures 2.4and 2.5). Coronal, sagittal, and cross‐sectional views are the recommended views for detecting vertical root fractures. One concern when evaluating for fractures is teeth that have been endodontically treated, as the filling material causes artifacts that obscure small fractures and create pseudo‐fracture lines ( Figure 2.6).
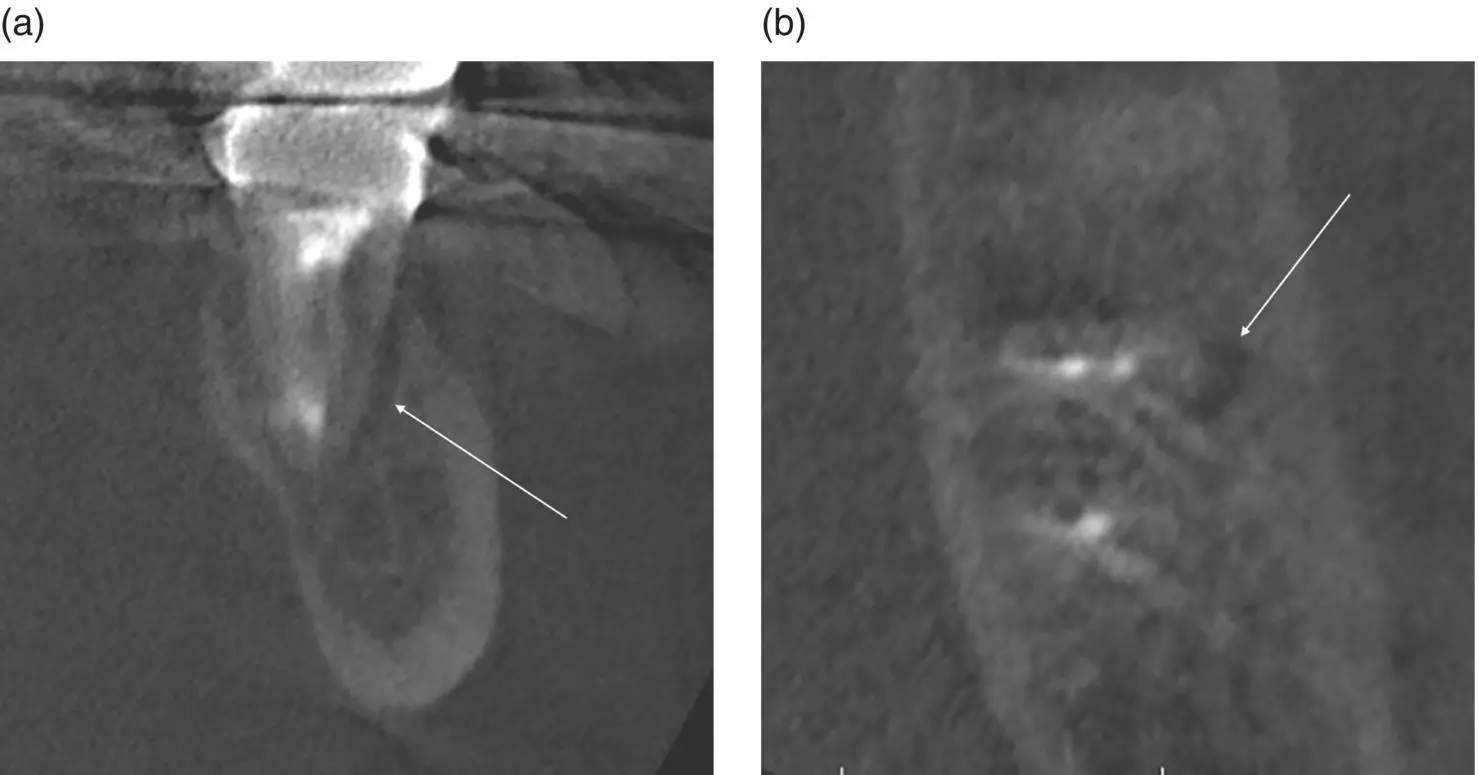
Figure 2.3. (a) Coronal view showing localized vertical bone loss (white arrow) along the facial root surface of a mandible molar. (b) Axial view showing localized bone loss (white arrow) along the facial root surface of a mandible molar.
Figure 2.4. (a) Pantomograph showing impacted maxillary right canine. (b) Periapical radiographs showing impacted maxillary right first premolar and canine with a dentigerous cyst. (c) Cross‐sectional slices showing a vertical root fracture on the maxillary right second premolar (white arrow) and dentigerous cyst associated with impacted canine.
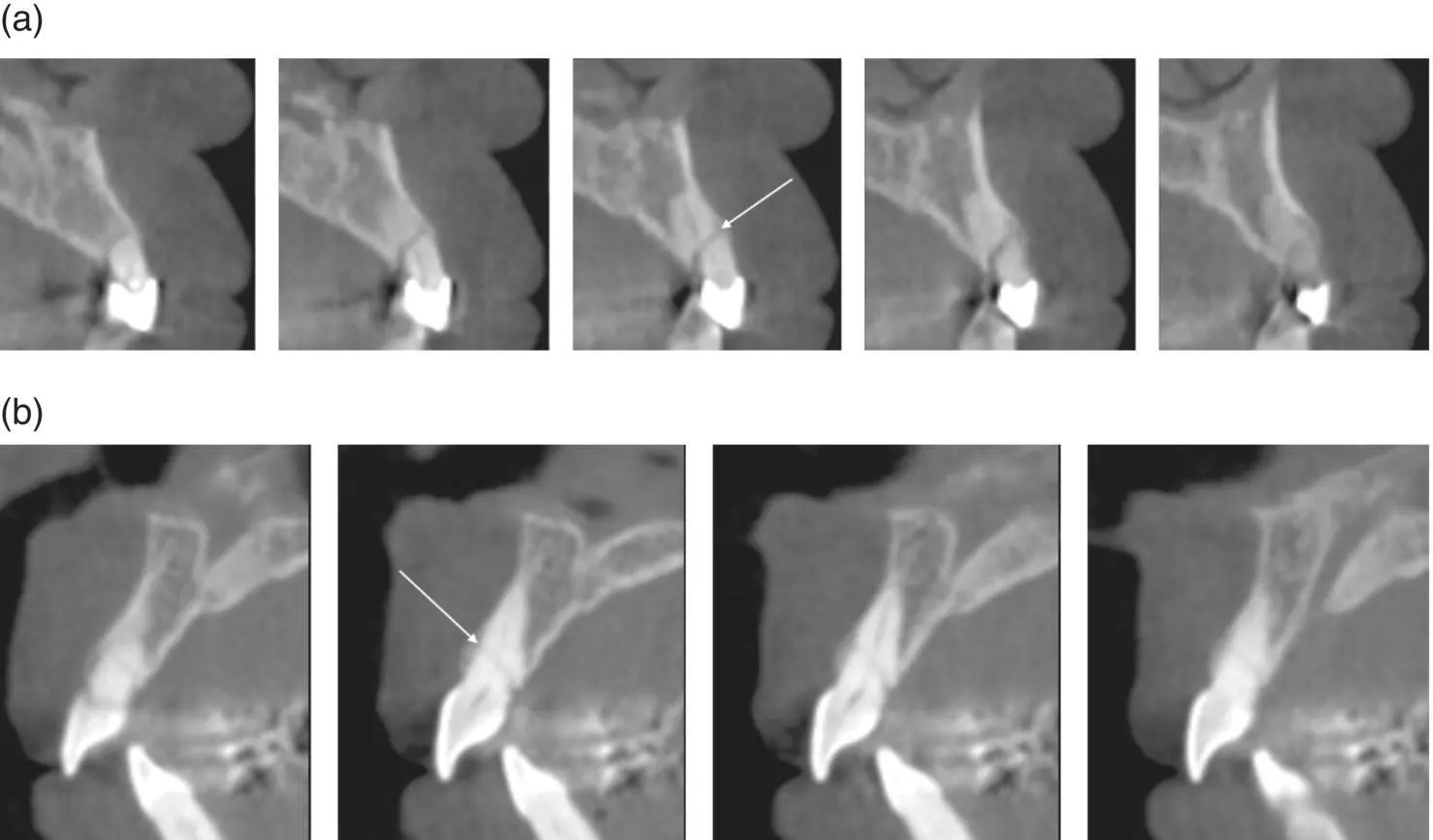
Figure 2.5. (a) Cross‐sectional slices showing a horizontal root fracture (white arrow). (b) Cross‐sectional slices showing a horizontal root fracture (white arrow).
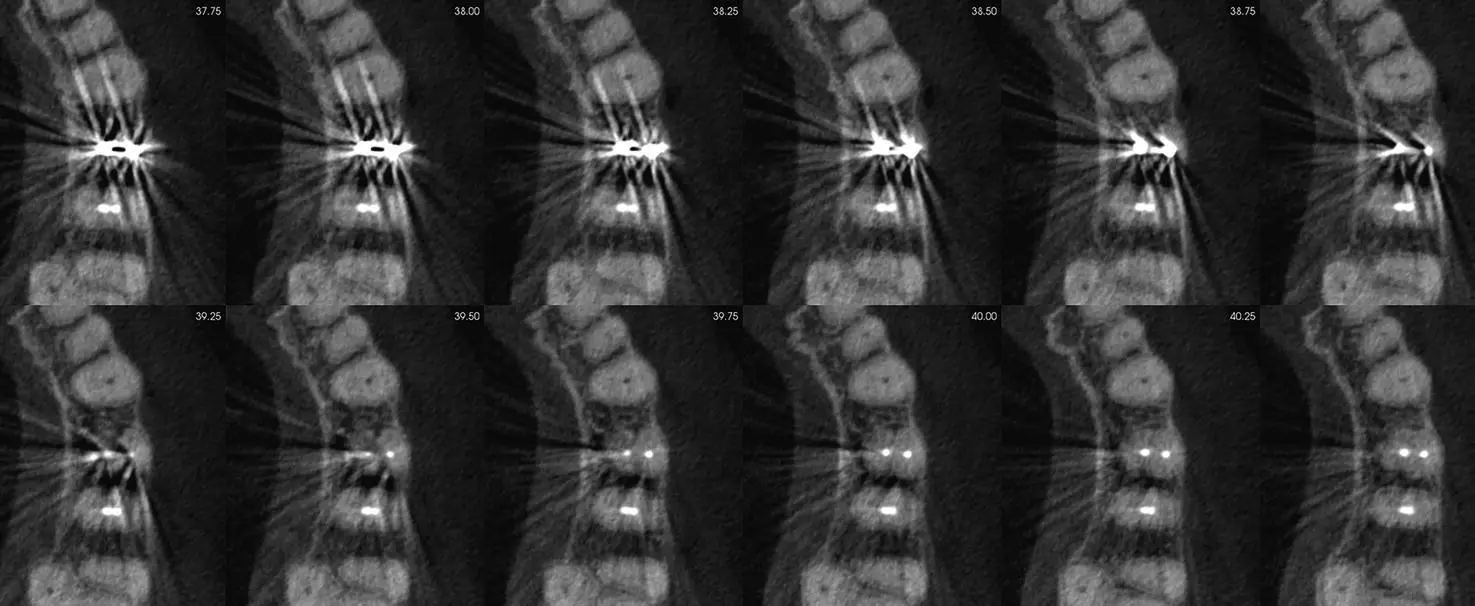
Figure 2.6. Axial views showing artifact streaking from an endodontically treated tooth obscuring the root when evaluating for root fractures.
The smallest root fracture that can be visualized on a CBCT scan is determined by the resolution/voxel size used. This is due to the Nyquist Theorem, which samples digitized information at 2 times the highest frequency. On a CBCT scan, this translates to the smallest root fracture visualized is twice the resolution/voxel size used. For example, if a resolution/voxel size of 0.2 mm is used, the smallest root fracture visible would be 0.4 mm.
7 = Limited FOV CBCT should be considered when evaluating nonhealing previous endodontic treatment.
8 = Limited FOV CBCT should be considered for nonsurgical retreatment.
Surgical Retreatment
9 = Limited FOV CBCT should be considered for presurgical treatment planning.
Special Conditions
10 = Limited FOV CBCT should be considered for implant treatment planning and placement.
11 = Limited FOV CBCT should be considered for diagnosis and management after trauma.
12 = Limited FOV CBCT should be considered for localizing resorption ( Figures 2.7and 2.8).
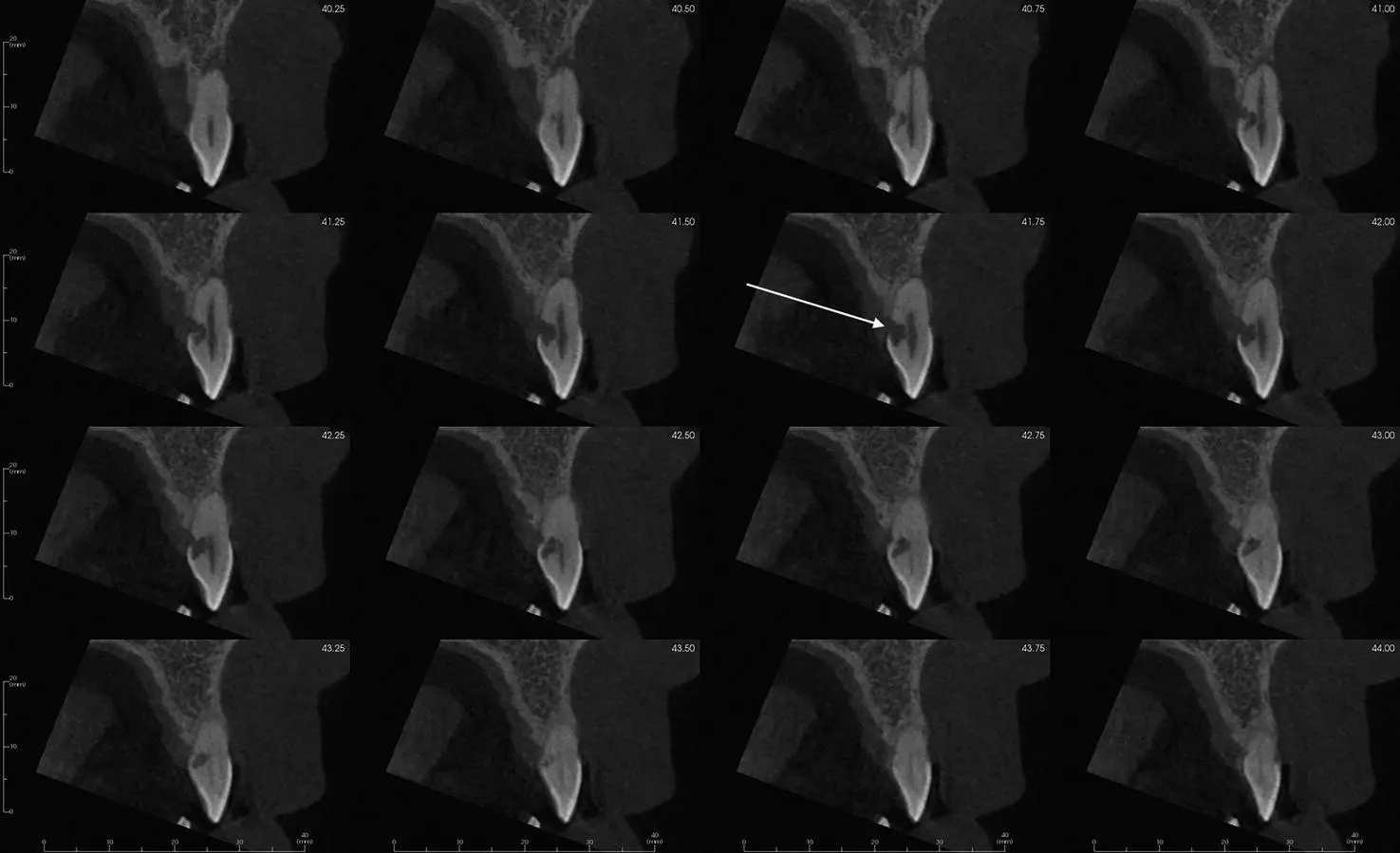
Figure 2.7. Sagittal views showing the extent of invasive cervical resorption (white arrow) on the palatal root surface of a maxillary incisor.
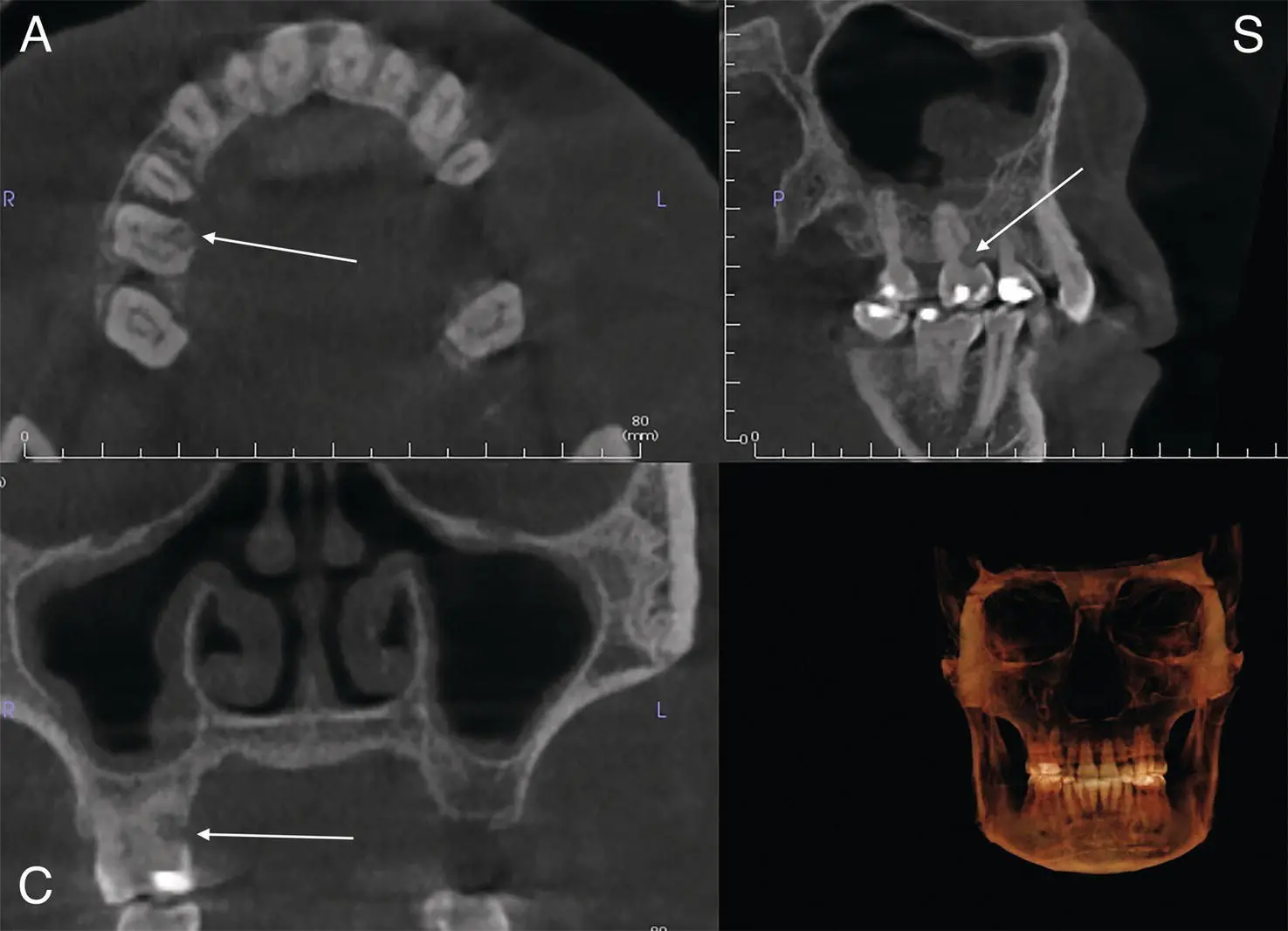
Figure 2.8. Axial (A), coronal (C) and sagittal (S) views showing the extent of palatal root resorption (white arrow) of the maxillary right first molar.
Outcome Assessment
13 = Intraoral radiographs should be considered when evaluating healing post‐nonsurgical or surgical endodontic treatment if no clinical signs or symptoms are present.
HOWEVER
14 = Limited FOV CBCT should be considered if it was used pretreatment to re‐evaluate the tooth endodontically treated ( Figure 2.9).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Interpretation Basics of Cone Beam Computed Tomography»
Представляем Вашему вниманию похожие книги на «Interpretation Basics of Cone Beam Computed Tomography» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Interpretation Basics of Cone Beam Computed Tomography» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.