Daniel Buser - 30 Years of Guided Bone Regeneration
Здесь есть возможность читать онлайн «Daniel Buser - 30 Years of Guided Bone Regeneration» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:30 Years of Guided Bone Regeneration
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
30 Years of Guided Bone Regeneration: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «30 Years of Guided Bone Regeneration»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
30 Years of Guided Bone Regeneration — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «30 Years of Guided Bone Regeneration», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
With transplantation of autogenous bone, bone-stimulating growth factors and viable osteogenic cells are brought to the recipient site. 86 The number of cells and the concentration of growth factors demonstrate great inter- and intraindividual variation and depend largely on patient’s age, presence of systemic diseases, and location of the donor site. The growth factors comprise BMPs, TGF-β, IGF, PDGF, and FGF. They are mainly present in the bone matrix and are released either passively or during resorption of the autografts. The higher the absolute surface area of the autograft, the faster the growth factors are set free. This means that blocks of cancellous bone release growth factors more readily than blocks of compact bone and that particulate autografts demonstrate faster release of bone-stimulating growth factors than do blocks. 87 More about growth factor release from autogenous bone grafts is discussed in chapter 3.
The cells of primary interest in GBR procedures are the osteogenic cells (ie, osteoblasts, bone-lining cells, preosteoblasts, and pluripotent stem cells). These cells are most numerous in trabecular bone and least numerous in compact bone. The osteogenic potential is greater in young healthy individuals than in elderly patients. This is mainly because of a decreased proliferative capacity of osteoprogenitor cells in older individuals, rather than due to compromised function of the osteoblasts. 88 The presence of living osteocytes in transplanted autogenous bone confirms that cells can survive the transplantation procedure, but whether transplanted osteocytes have a function in bone formation is as little known as what this function may be. As discussed previously, osteocytes play a very important role in bone physiology.
Autografts can be harvested at different intraoral or extraoral locations ( Table 2-1) and can be used in different forms ( Table 2-2). 89 Both autografts and bone substitute materials can be used as block grafts, which are beyond the scope of this chapter, or as particulate grafts.
Table 2-1Donor sites for autografts
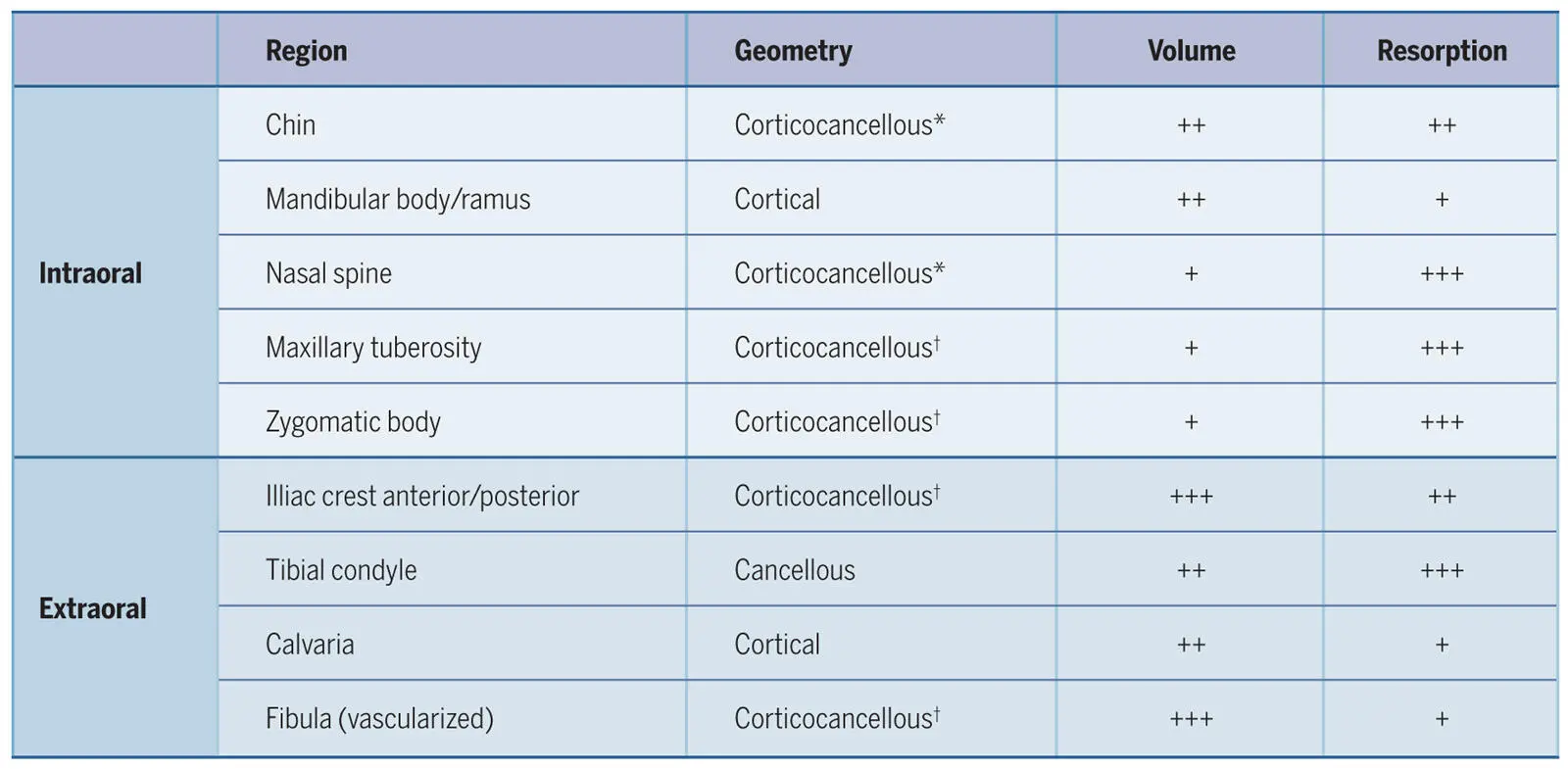
*More cortical than cancellous bone
†More cancellous than cortical bone
+, Sufficient bone for augmenting a single-tooth gap; ++, sufficient bone for up to two sinus augmentations; +++, sufficient for major inlay and onlay augmentations and reconstruction of continuity defects.
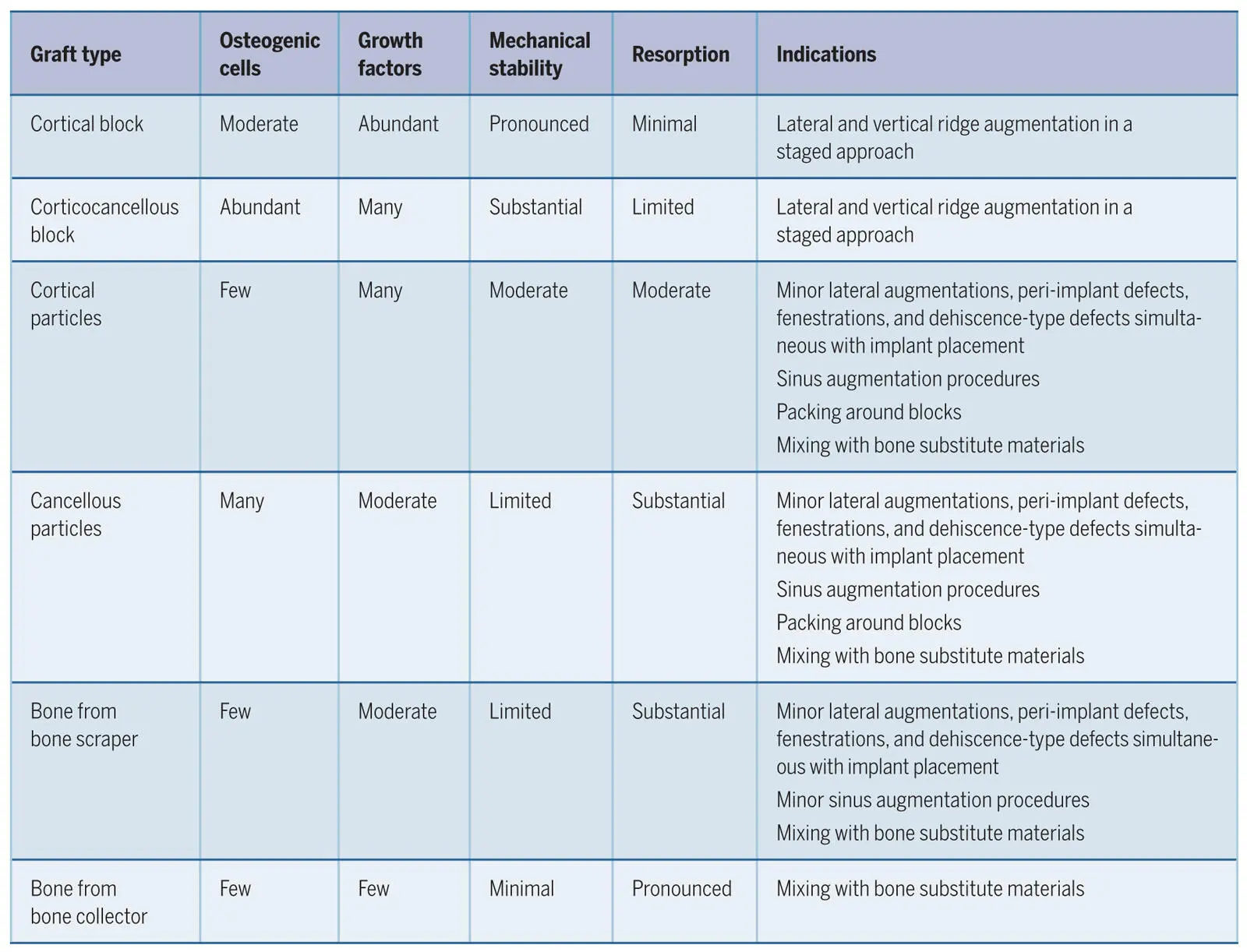
Table 2-2Characteristics of autografts and their indications
Autogenous particulate grafts
Bone particles are usually applied in an area where there is no need for mechanical strength, such as in peri-implant bone defects or in sinus floor elevation procedures. Particulate bone can be harvested either directly with a bone scraper (bone chips), with a piezoelectric device, with a bone collector (bone slurry or dust), or indirectly from a harvested bone block that is ground in a bone mill. The higher the relative surface area, the greater the osteoconductive and osteoinductive potential of autogenous bone. This is because the greater surface area allows more passive release of growth factors and more active liberation of growth factors by osteoclasts while they resorb the bone matrix. 87 While the osteopromotive potential of an autograft increases when it is particulated, the total number of intact osteogenic cells decreases through mechanical graft manipulation. 90 The smaller the particles, the more the stability of the graft decreases. In addition, the resorption rate increases considerably. 91 In a recent preclinical study, bone chips, bone slurries, bone harvested with a piezoelectric device, and bone ground by a bone mill were tested for their ability to support bone healing in defects created in the mandible of minipigs and covered with an ePTFE membrane. 92 The results showed that all bone defects healed with the same amount of new bone, regardless of the harvesting procedure and of the healing period (Fig 2-23). The highest number of osteoclasts was found after 1 to 2 weeks on the bone slurries, confirming that smaller particles trigger increased resorption (Fig 2-24).
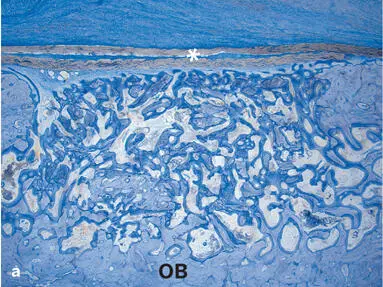
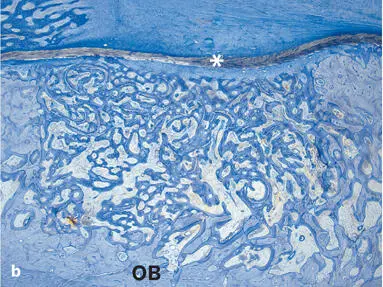
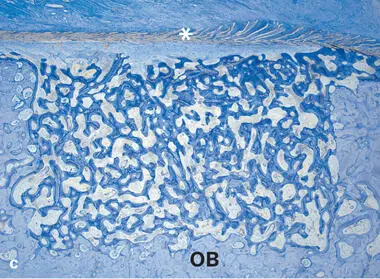
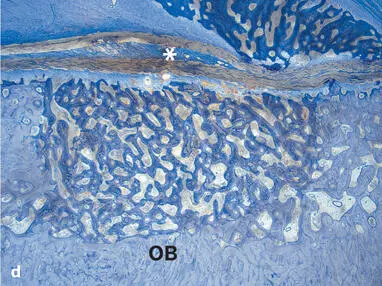
Fig 2-23Histologic sections illustrating standardized bone defects in the minipig mandible (undecalcified ground sections; toluidine blue stain). Old bone (OB) and an ePTFE membrane (asterisks) delineate the defects. The defects were filled with autogenous bone. (a) Particulate from corticocancellous bone with a bone mill. (b) Bone chips harvested with a bone scraper. (c) Bone particles harvested with a piezoelectric instrument. (d) Bone slurry from a bone trap filter. After 4 weeks of healing, all types of autogenous bone grafts are embedded in a trabecular network of new bone that completely fills the defect areas.
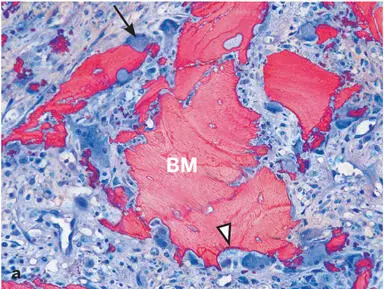

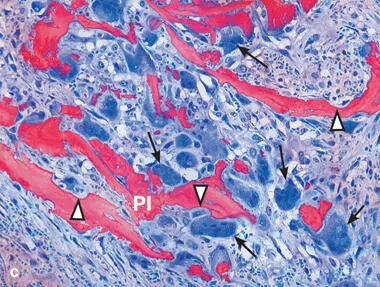
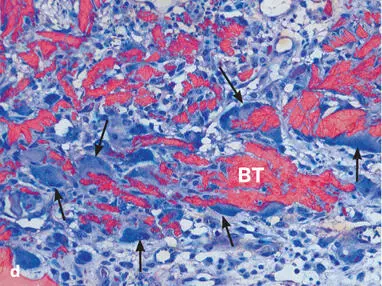
Fig 2-24Histologic sections 1 week after implantation resorption of autogenous bone. (a) Particulate from corticocancellous bone with a bone mill (BM). (b) Bone chips harvested with a bone scraper (BS). (c) Bone particles harvested with a piezoelectric instrument (PI). (d) Bone slurry from a bone trap filter (BT). All harvesting techniques show numerous Howship lacunae (arrowheads) and osteoclasts (arrows) . The lowest number of osteoclasts is found on BM particles, and the highest number is found on BT particles.
A vast body of scientific evidence from experimental and clinical studies documents the suitability of particulate autografts for bone augmentation procedures when a highly osteogenic graft is needed. Nevertheless, the advantages and disadvantages of the different harvesting procedures in the context of clinical applications need to be discussed.
Autogenous bone from bone collectors.With this harvesting method, bone dust is collected through a filter that is connected to the suction device used during preparation of the implant bed. The philosophy is intriguing, because the acquisition of the autogenous bone graft causes no additional discomfort for the patient, but several disadvantages exist. Viable cells are clearly present in lower numbers than in other autografts, 90 , 93 the amount of bone that can be collected can only cover small peri-implant defects, and contamination of the graft with bacteria from the oral cavity occurs frequently. 94
Читать дальшеИнтервал:
Закладка:
Похожие книги на «30 Years of Guided Bone Regeneration»
Представляем Вашему вниманию похожие книги на «30 Years of Guided Bone Regeneration» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «30 Years of Guided Bone Regeneration» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.